CASE REPORT
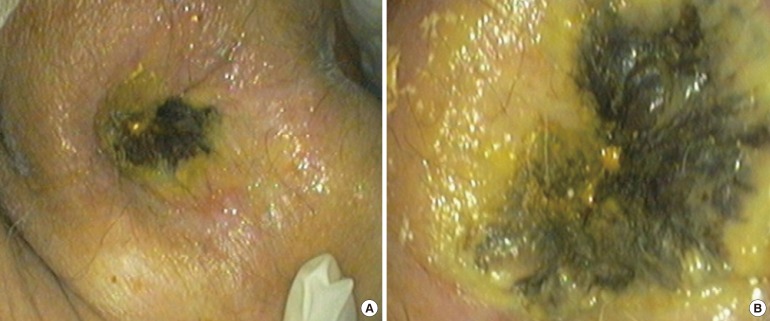
An 83-year-old male presented to the Emergency Department with a 2-day history of diarrhea without blood. Past medical history included Alzheimer disease, arterial hypertension and diabetes mellitus (well controlled with insulin, but with known microvascular complications - retinopathy and nephropathy). Clinical information was provided by the caregivers because the patient was not communicative. They denied any history of trauma or topical medications. The patient was dehydrated and hypotensive. Abdominal exam was normal. Anal inspection revealed a darkened color of the anoderm (Fig. 1). Digital rectal examination was painful, with apparent hypotony of the anal sphincter, no palpable masses and no blood. Lymphadenopathy was absent.
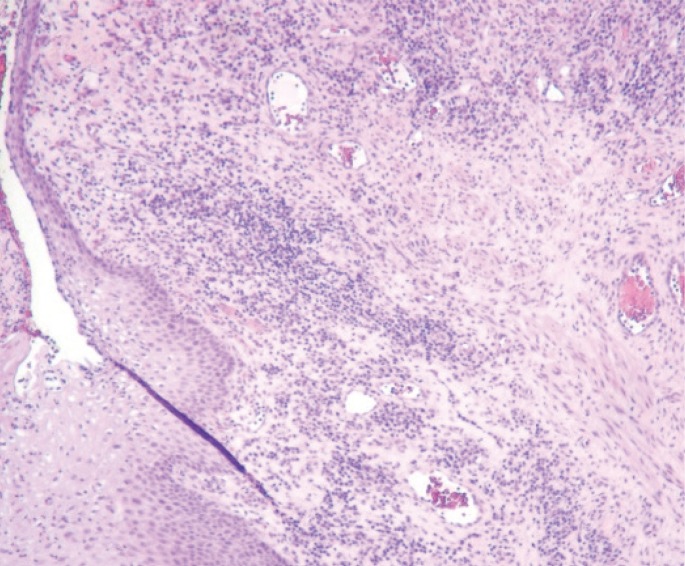
Laboratory results revealed the following: leukocytes (16,000/┬ĄL; 4,000ŌĆō10,000/┬ĄL), C-reactive protein (101.6 mg/L; <5 mg/L); creatinine kinase (346 U/L; <250 U/L); lactate dehydrogenase (196 U/L; 50ŌĆō115 U/L). Flexible sigmoidoscopy showed a circumferential darkening of the anal canal (total distance of 25 mm), with a proximal margin 2 mm below the dentate line and a normal rectal mucosa with brown molded feces inside the rectum (Fig. 2). Histopathology showed a polymorphic inflammatory infiltrate, with extensive necrosis and ulceration up to the hypodermis (Fig. 3). Microbiology was negative. No imaging study, such as computed tomography, magnetic resonance, endoanal ultrasound, or angiography, was performed due to the patient's performance status. Anal sphincter function was not evaluated because the patient was not cooperative.
After admission, diarrhea was no longer observed. Hypotension quickly improved after fluid therapy with normalization in the first 2 hours after admission. Anal lesions were not improved after 5 days of medical therapy (broad-spectrum parenteral antibiotics and intravenous fluids). On day 6 after admission, surgical debridement with superficial necrotic tissue removal and hemostasis with an absorbable haemostatic gelatin sponge was performed. During surgery, gangrenous superficial tissues were noticed, but muscular tissue and the anal sphincter were spared. The patient's perianal findings were clearly improved 5 days after surgical treatment (Fig. 4). After 10 months of follow-up, neither cutaneous lesions nor fecal incontinence had occurred.
DISCUSSION
Ischemia of the anal region is rare because this region has a very rich vascularization [1,2,3,4]. The anal canal is supplied by the inferior, middle and superior rectal arteries, which communicate between themselves and with branches of the lumbar, internal iliac and inferior vesical arteries [1,2,3,4]. The hemorrhoidal plexus drains the superior rectal (portal circulation) and the middle and inferior rectal veins (systemic circulation), establishing an important portosystemic anastomotic network [1,3,4]. An extensive search in the literature revealed a single case of anal sphincter necrosis as a result of an electric current injury [5], 2 cases of anorectal necrosis secondary to hemorrhoidal sclerotherapy [6,7] and 2 cases of anorectal necrosis after paracetamol suppository abuse [8,9].
Cases of rectal and anal ischemia almost invariably include risk factors such as advanced age, atherosclerotic disease, arterial hypertension or diabetes mellitus [1,2,10]. Other causes of rectal ischemia include embolization during angiography, hemorrhoid infection, vasculitis, systemic lupus, radiotherapy, and phosphate enema application [1,11,12,13,14,15]. Sometimes, no precipitating event can be identified [1]. In our case, the hypoperfusion hypothesis seems to be the most plausible explanation because the patient had arterial hypotension and microvascular complications of diabetes mellitus. In addition, the patient's malnutrition and frailty compromised the barrier and healing mechanisms. Despite the absence of any reference, the possibility of chemical or traumatic injury cannot be excluded. Diarrhea was attributed to transient anal incontinence upon ischemia. This hypothesis is further supported by the absence of diarrhea after admission and by the presence of solid feces in the lumen during the flexible sigmoidoscopy. The patient's recovery after surgical treatment was favorable, as a clear improvement in the lesions was noted.
Spontaneous anal necrosis is an apparently unknown clinical entity, with no similar cases having been discussed in the literature until now. This case underlines the importance of a detailed physical examination to reach the correct diagnosis.