INTRODUCTION
Several studies have revealed that a laparoscopic colorectal resection not only reduces postsurgical pain and the recovery time, but it is also oncologically safe, and indications for its use are expanding gradually [1-3]. Nevertheless, the results of long-term follow-up have not been reported abundantly, but recently, Clinical Outcomes of Surgical Therapy (COST) [4-7], Conventional versus Laparoscopic-Assisted Surgery in Colorectal Cancer (CLASICC) [5], Colon Cancer Laparoscopic or Open Resection (COLOR) [6] and other large-scale studies have reported the outcomes, including the three-year, the five-year and the disease-free survival rates, of long-term follow up after laparoscopic surgery. Nevertheless, outcomes for rectal cancer are not abundant, and, in large scale studies, were included only in the CLASICC study [5]; thus, more studies on rectal cancer are required [3]. We performed laparoscopic resections on colorectal cancer patients, including patients with rectal cancer, examined the long-term follow-up results, and assessed the oncological outcomes and safety of laparoscopic colorectal resections.
METHODS
Between January 2001 to December 2003, 303 patients who were diagnosed as having colorectal cancer and who underwent a laparoscopic resection at our hospital, excluding 3 cases that were converted to open abdominal surgery due to failure of end-to-end anastomosis devices or perforation of tumors, were included. Using prospectively collected data, we examined gender, age, disease stage, and postoperative complications. Local and distant metastases, the five-year survival rate, and the five-year disease-free survival rate were examined in 271 patients who could be followed for longer than 36 months or in whom recurrence or death was confirmed before 36 months. The follow-up periods were calculated based on the last visit to the outpatient clinic, and for cases who did not visit our hospital, telephone interviews and mortality data from the Bureau of Statistics were used.
Postoperative chemotherapy was administered according to the stage. For stage II, 5-fluorouracil (5-FU) oral medications were administered for 6 months to 1 year and for stage III, injection of 5-FU and leucovorin were infused continuously for 5 days; the regimen was repeated 6 times at 28-day intervals. Preoperative radiation therapy was performed for stage T4 male patients whose lesions were located below the mid rectum or for cases in which sphincter preservation was required. Radiation therapy was performed after surgery for cases whose lateral resection margin was positive or for cases whose resection margin was as close as within 0.5 cm of the distal resection margin or for cases with advanced cancer higher than N2. Radiation therapy patients received a total of 4,500 cGy, 180 cGy per day for 5 weeks (25 times). Outpatient clinic follow-up was performed every 3 months, with blood test, chest X-ray and abdominal computed tomography (abdominal CT) being performed every 6 months for up to 3 years and colonoscopic examination being performed annually for up to 5 years. For patients with higher than stage III cancer, chest computed tomography was performed annually.
For statistical analysis of the overall survival rate and the disease-free survival rate, the Kaplan-Meier method was applied using the SPSS ver. 11.0 (SPSS Inc., Chicago, IL, USA). Significance was validated by using the log-rank test and P-values less than 0.05 was considered to be significant.
RESULTS
Clinical characteristics of the patient group
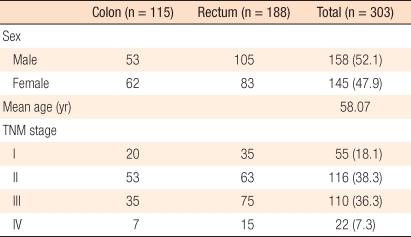
Of the total 303 patients, 158 (52.2%) were male, and 145 (47.9%) were female; their mean age was 58 years. Regarding tumor site, the colon was the site in 115 patients (38.0%), and the rectum was the site in 188 patients (62.0%). In regard to the distribution according to the disease stage of the tumor, stage I tumors were present in 55 patients (18.2%), stage II in 116 patients (38.3%), stage III in 110 patients (36.3%), and stage IV in 22 patients (7.2%). In colon cancer, stage II tumors were present in 53 patients, which was the most prevalent. In rectal cancer, stage III tumors were present in 75 patients, which was the most prevalent (Table 1). Thirty-two patients (10.6%) whose outpatient follow-up was terminated within 36 months after surgery were excluded from the analysis of survival rate and recurrence rate. Of those 32 patients, 78.1% had stage I and stage II tumors (9 cases [28.1%] and 16 cases [50.0%], respectively), 18.8% had stage III tumors (6 patients), and 18.8% had stage IV tumors (1 patient). Among stage IV patients, a curative resection was possible for 2 patients; for the other patients, palliative treatments were performed.
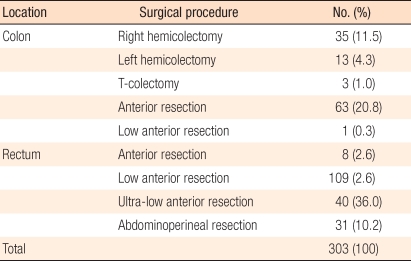
In regard to the type of surgery for colon cancer patients, a right hemicolectomy was performed on 35 patients, a left hemicoloctomy was performed on 13 patients, a transverse colectomy was performed on 3 patients, and an anterior resection was performed on 63 patients. For rectosigmoid colon cancer, a low anterior resection was performed on 1 patient. In rectal cancer patients, an anterior resection was performed on 8 patients, a low anterior resection was performed on 109 patients, an ultra-low anterior resection was performed on 40 patients, and an abdominoperineal resection was performed on 31 patients (Table 2).
For rectal cancer patients, preoperative chemoradiation therapy was performed on 6 patients, and postoperative radiation therapy was performed on 17 patients. Those patients included one colon cancer patient and 16 rectal cancer patients. One colon cancer patient received chemoradiation therapy after a tumorectomy because of an isolated tumor at the pelvic wall. Adjuvant chemotherapy was performed on 245 patients (80.9%), intravenous chemotherapy was performed on 33 colon cancer patients and 66 rectal cancer patients. Oral administration was performed on 56 colon cancer patients and 90 rectal cancer patients.
Operative data
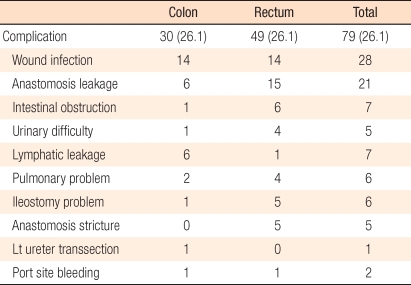
In colon cancer patients, the mean operation time was 180 minutes (range, 100 to 355 minutes), and in rectal cancer patients, it was 212 minutes (range, 120 to 535 minutes). The mean blood-loss volumes during surgery for colon and rectal cancer patients were, respectively, 99 mL (range 20 to 700 mL) and 96 mL (range, 30 to 1,200 mL). The average hospital stay period was 11 days (range, 6 to 46 days). The average follow-up period was average 54 months (range, 0.5 to 92 months). The average numbers of resected lymph nodes in colon and rectal cancer patients were 26 (range, 4 to 65) and 21 (range, 0 to 63), respectively. In colon and rectal cancer patients, the lengths of the distal resection margins were 10.1 cm (range, 1.5 to 41 cm) and 2.7 cm (range, 0.2 to 13.2 cm), respectively. One rectal cancer patient presented with invasion to the distal or radical resection margin, with invasion toward the vagina (Table 3). Postoperative complications developed in 79 patients (26.1%) and wound infections in 28 patients (9.2%), which were the most prevalent. Anastomosis leakage occurred in 21 patients (6.9%), 6 colon cancer patients and 15 rectal cancer patients. Among them, 2 of the 6 colon cancer patients and 12 of the 15 rectal cancer patients received an ileostomy; the remaining patients improved with conservative treatments. The symptom of ileus developed in 7 patients (2.3%), and most patients improved with conservative treatment. In one patient, a bandlysis operation was performed (Table 4).
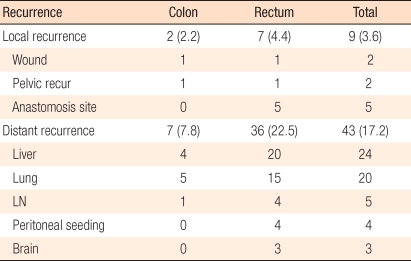
Recurrence and survival rates
The five-year survival rate was examined in 271 patients who were followed for longer than 36 months. The recurrence rate and the five-year disease-free survival rate were examined in 250 patients, excluding stage IV patients, in order to select patients for whom a curative treatment had been offered. Local recurrences were shown in nine cases (3.6%). In two patients, recurrence occurred at the main incision site of the tumor extraction resection area, in five patients, it occurred at the pelvic wall and in two patients, it occurred at the anastomosis site. Among the two patients with anastomosis-site recurrence, an abdominoperineal resection was performed on one patient, and conservative treatments were used for the other. According to the location of the tumor, two local recurrences developed in colon cancer patients (2.2%), and seven local recurrences developed in rectal cancer patients (4.4%). Concerning the TNM stage, stage I cancer was present in one patient with anastomosis-site reccurrence, stage II cancer in three patients, and stage III cancer in five patients. Distant metastases occurred in 43 of the 250 patients (17.2%) for whom the recurrence and the five-year disease-free survival rates had been examined. Liver metastasis occurred in 24 of those patients, lung metastasis in 20, lymph node metastasis in 5, peritoneal metastasis in 4, and brain metastasis in 3. Regarding the location of the tumor, colon cancer was present in 7 patients (7.8%) and rectal cancer in 36 patients (22.5%). Concerning the distribution of the TNM stage, stage I cancer was present 3 patients, stage II in 7 patients, and stage III in 33 patients (Table 5).
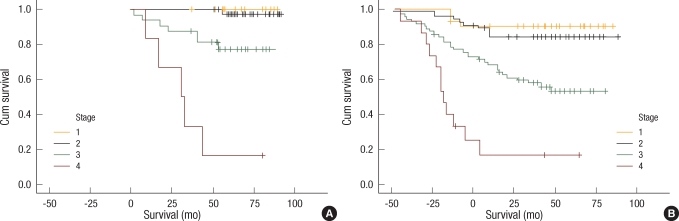
The five-year survival rate of all patients was 73.7%. In colon cancer patients, it was 86.1%, and in rectal cancer patients, it was 68.8%, so the five-year survival rate was shown to be lower in rectal cancer patients. In colon cancer patients, the five-year survival rate was 100% for stage I patients, 97.6% for stage II patients, 77.5% for stage III patients, and 16.7% for stage IV patients. In rectal cancer patients, the five-year survival rate was 90.2% for stage I patients, 84.0% for stage II patients, 57.6% for stage III patients, and 13.3% for stage IV patients (Table 6, Fig. 1). The five-year disease-free survival of all patients was 80.1%. For colon cancer patients, it was 89.8%, and for rectal cancer patients, it was 74.5%. According to TNM disease stage, in colon cancer patients, The five-year disease-free survival rates were 100%, 97.7%, and 74.2% for stage I, II, and III patients, respectively. In rectal cancer patients, the five-year disease-free survival rates were 90.0%, 83.9%, and 59.2% for stage I, II, and III patients, respectively (Table 6, Fig. 2).
DISCUSSION
In colorectal cancer, laparoscopic surgery was introduced in the 1990s. In the initial period, the recurrence rate at the incision site was reported to be high, and application of laparoscopic surgery to malignant tumors was accepted negatively. Nevertheless, with the development of laparoscopic equipment and its supporting techniques, gradually, the laparoscopic colectomy could be performed safely. Recently, laparoscopic surgical methods have been applied frequently to malignant tumors [8-10]. In the 2000s, results of randomized large-scaled studies have been reported, and the laparoscopic colectomy was shown to be oncologically safe. Results of studies that examined the recurrence and the survival rates in long-term follow up led to its being generally accepted as oncologically safe [4-7].
In our study, long-term oncological safety was assessed by examining postoperative results, such as the resection margin, the number of resected lymph nodes, and complications, as well as the recurrence and the survival rates of patients who were available for long-term follow up. The average distal resection margin was 5.59 cm, one case showed invasion to the radical resection margin, and the average number of resected lymph nodes was 22.5. These findings demonstrated that oncologic safety of our laparoscopic surgery was comparable to open surgery or to previous results of other laparoscopic surgery groups [11, 12].
In the results of most studies reported recently, the recurrence rate after laparoscopic surgery for colorectal cancer was shown to be comparable to or better than that of open abdominal surgery [5-7, 13]. In our study, the local recurrence rates were 3.6% for all patients, 2.2% for all colon cancer patients and 4.4% for all rectal cancer patients. The distance recurrence rates were 17.2% for all patients, 7.8% for colon cancer patients, and 22.5% for rectal cancer patients. Both recurrence rates were higher when the tumor was located in the rectum. The results were not greatly different from those in the study reported by Kim et al. [14], who examined the recurrence rate after performing open abdominal surgery on colorectal cancer patients on whom a radical resection could be performed. In that study, the local recurrence rates were 3.1% and 7.2% in colon cancer and rectal cancer patients, respectively. The distant recurrence rates were 10.5% and 17.9% in colon cancer and rectal cancer patients, respectively. In the CLASICC trial, which studied patients who were available for longer than 3 years of follow up after a colorectal resection, the local recurrence in colon cancer patients was 7.3%, and in rectal cancer patients, it was 9.7%; the distant recurrence rates were 11.3%, and 18.6% in colon cancer and rectal cancer patients, respectively. Our results revealed that the total local recurrence rate and the distant recurrence rate for colon cancer patients were lower compared with CLASSIC trial, but the distant recurrence rate for rectal cancer patients was slightly higher. This is thought to be related to the characteristics of the rectal cancer patient group, in that the incidence of lower rectal cancer was higher than that of upper rectal cancer. In other results reported by Kim et al. [15] for a study conducted on rectal cancer patients, the distant recurrence rates in the upper, middle and lower rectum were 17%, 18%, and 20%, respectively, and these results according to the location of tumor for rectal cancer are comparable to our results.
Reviewing the results of long-term follow up conducted in other countries, the three-year survival rates in large-scaled prospective studies, such as the COST study [5], the CLASICC trial [6], and the COLOR study [7], were 85%, 66.7%, and 84.2% for open surgery and 85%, 68.4%, and 84.2% for laparoscopic surgery, respectively. Among them, the CLASICC study included rectal cancer [6]; thus, the survival rate was lower than those of other studies. The COST study [5] reported that the five-year survival rate to be 74.6% in the open surgery group and 76.4% in the laparoscopic surgery group, but rectal cancer was not included. In other studies, the average five-year survival rates for colon cancer treated laparoscopically were 77%, 100-61.6% (stage I-III), and 65.3% [16-18, respectively]. In our study, the average five-year survival rate was 73.7%, and the five-year disease-free survival rate was 80.1%, which are comparable to previous results for open abdominal surgery or to the results of other laparoscopic surgeries. Korean reports on long-term survival are not abundant. In regard to open abdominal surgery, in the study reported by Kim et al. [14], the five-year survival rate for colorectal cancer patients was shown to be 61.5%. In the results of Moon et al. [19], which reported the long-term follow-up outcomes for longer than 10 years, the average five-year survival rate in colorectal cancer cases was 77.6%, and the five-year disease-free survival rate was 77.5%. In regard to the results for laparoscopic surgery, in the study reported by Lee et al. [20] in 2008, the three-year disease-free survival rate for colon cancer patients was 89.2%, and the three-year disease-free survival rate for rectal cancer patients was 85.7%.
In rectal cancer, in comparison with colon cancer, a noticeably poor survival rate or recurrence rate has been reported in many studies. The blood flow of the rectum is thought to be different from that of the colon; thus, the recurrence pattern is different. Another reason is that the surgery for rectal lesions is difficult because of the location itself. Recently, surgery outcomes for rectal cancer have improved greatly, which is thought to be influenced by the application of the concept of total mesorectal excision (TME) to rectal surgery. In laparoscopic rectal cancer, whether a good surgical view is secured and whether a TME is sufficiently achieved are thought to be factors that may exert influences on the outcome of long-term follow up after surgery for rectal cancer [21]. Although not multicenter studies, some studies have reported the results of long-term follow up after laparoscopic rectal cancer resection. In the study reported by Lezoche et al. [22], which presented the results of long-term follow up for an average of 78 months, the average survival rate was shown to be 71%. In the study reported by Sample et al. [17], for which the average follow-up period was 35.8 months, and in the study reported in Japan by Kitano et al. [23] in 2006, long-term outcomes were reported. In regard to studies reported in Korea, in the study reported by Lee et al. [20], with an average 35-month follow up, after laparoscopic surgery for rectal cancer, the three-year disease-free survival rate was 85.7%. The average three-year survival rate reported by us in 2006 was 88.9%, and the three-year disease-free survival rate was 78.8% [24]. According to the study reported by Lee et al. [25] in 2007 for 251 rectal cancer patients with preoperative chemoradiation therapy, the five-year survival rate after open abdominal surgery was 93.0% for stage I cancer, 90.3% for stage II cancer, and 76.1% for stage III cancer. In our study of rectal cancer patients, preoperative chemoradiation therapy was not common; nonetheless, the overall five-year survival rate was 90.2% for stage I cancer, 84.0% for stage II cancer, and 57.6% for stage III cancer, and the local recurrence rate was 4.4%, which are comparable to the results of a study reported by Kim et al. [15], who examined long-term follow-up outcomes after open abdominal surgery. In addition, recently, the indications for preoperative chemoradiation therapy have been extended; hence, if preoperative or postoperative chemotherapy is administered properly, better results may be obtained. The five-year survival rate for laparoscopic rectal surgery in Korea has not been reported. Thus, this study, which included a high ratio of rectal cancer patients with long-term follow-up results, confirmed the safety of the laparoscopic resection for the treatment of rectal cancer.
Since our study was conducted only on patients for whom long-term follow-up was possible, 32 patients (10.6%) were excluded from the study. Other studies that performed long-term follow up and assessed the outcomes have reported that follow up was interrupted in 2-12% of all cases [7, 15, 16]. In our study, 78.1% of all patients were stage I and stage II patients; thus, patients with an early stage of the disease comprised a large part of the excluded patient population. Nevertheless, selection bias may have been present, so a more systemic management of the postoperative follow-up protocol is required.
In this study, the long-term results for a laparoscopic colorectal resection over an average of 57 months, including the five-year survival rate, the five-year disease-free survival rate, and the recurrence rate, were acceptable in comparison with those for open abdominal surgery. Laparoscopic surgery for the treatment of colorectal cancer is thought to be a good alternative to open surgery, with tolerable oncologic long-tem results.