Only the Size of Resected Polyps Is an Independent Risk Factor for Delayed Postpolypectomy Hemorrhage: A 10-Year Single-Center Case-Control Study
Article information
Abstract
Purpose
A colonoscopic polypectomy is an important procedure for preventing colorectal cancer, but it is not free from complications. Delayed hemorrhage after a colonoscopic polypectomy is one infrequent, but serious, complication. The aim of this study was to identify the risk factors for delayed hemorrhage after a colonoscopic polypectomy.
Methods
This was a retrospective case-control study based on medical records from a single gastroenterology center. The records of 7,217 patients who underwent a colonoscopic polypectomy between March 2002 and March 2012 were reviewed, and 92 patients and 276 controls were selected. Data collected included comorbidity, use of antiplatelet agents, size and number of resected polyps, histology and gross morphology of resected polyps, resection method, and use of prophylactic hemostasis.
Results
The average time between the procedure and bleeding was 2.71 ± 1.55 days. Univariate and multivariate analyses revealed that the size of the polyps was the only and most important predictor of delayed hemorrhage after a colonoscopic polypectomy (odds ratio, 2.06; 95% confidence interval, 1.12-1.27; P = 0.03).
Conclusion
The size of resected polyps was the only independent risk factor for delayed bleeding after a colonoscopic polypectomy. The size of a polyp, as revealed by the colonoscopic procedure, may aid in making decisions, such as the decision to conduct a prophylactic hemostatic procedure.
INTRODUCTION
A colonoscopic polypectomy significantly reduces the incidence of colorectal cancer and cancer-related mortality [1, 2, 3, 4], but it is accompanied by several complications. Of these, hemorrhage is the most common complication [5, 6, 7, 8, 9, 10]. Delayed hemorrhage following a polypectomy occurs between 3 to 7 days after the procedure, and its incidence is commonly reported to range between 0.6% and 0.9% [5, 6, 7, 8, 9]. Postpolypectomy delayed hemorrhage is unpredictable and can occur after hospital discharge; therefore, it requires attention. Some retrospective case-control studies have endeavored to identify the risk factors associated with delayed hemorrhage after a colonoscopic polypectomy [11, 12, 13, 14, 15] and have indicated that the size, shape, and location (right hemicolon) of the polyp, a sessile polyp type, and the endoscopist's experience are the key risk factors for delayed postpolypectomy hemorrhage [11, 12, 13, 14, 15]. Our center carried out a ten-year single-center case-control study to identify the risk factors associated with delayed postpolypectomy hemorrhage.
METHODS
Study population and design
The study retrospectively examined the medical records of patients who underwent a colonoscopic polypectomy at a single gastroenterology center at Chungnam National University Hospital of Korea from March 2002 to March 2012. Delayed postpolypectomy hemorrhage was defined as the more than one occurrence of overt bleeding per anus or as a decrease in hemoglobin of more than 1 g/dL starting at least 6 hours after the colonoscopy. The case group consisted of patients who had undergone a delayed postpolypectomy; each delayed hemorrhage case had also undergone a therapeutic colonoscopy. The control group consisted of patients who had undergone an uncomplicated polypectomy 7 days earlier.
Among the 8,327 patients who had undergone a colonoscopic polypectomy, delayed postpolypectomy hemorrhage occurred in 92 patients. From the 8,235 remaining patients (8,327-8,392), we selected 276 patients for the control group, triple the number of patients experiencing postpolypectomy hemorrhage. For sampling, we applied a random sample extraction method. We categorized the hemorrhage group and the control group according to gender and age (less than 29 years old/30-39 years old/40-49 years old/50-59 years old/more than 70 years old); then, we applied a serial number to each category [12, 13, 14].
Methods
The risk factors for delayed hemorrhage were classified according to the patient, polyp, and procedure. Patient-related factors consisted of age, sex, comorbidity (hypertension, diabetes mellitus, cerebral vascular accident, coronary heart disease), and use of antiplatelets. Polyp-related factors included the size, number, location, and gross morphology of the polyp, and histologic findings. The sizes of the polyps were measured based on the sizes reported in the biopsy results. The locations of the polyps were divided into right (cecum, ascending colon) and left (transverse colon, descending colon, sigmoid colon, and rectum). The gross morphologies of the polyps were classified as pedunculated, semipedunculated, and sessile according to the presence or absence of a stalk. Histologically, the polyps were classified as hyperplastic polyps, adenomas, and adenocarcinomas. Procedure-related risk factors included resection methods (snare polypectomy or endoscopic mucosal resection) and use of prophylactic hemostasis.
Statistical analysis
Statistical analyses were performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). Categorical data were presented as frequencies and were compared using chi-square statistics or the Fisher exact test. Continuous data were presented as means ± 1 standard deviation and were compared using the Student t-test. Independent predictors for the occurrence of delayed postpolypectomy hemorrhage were determined using a multivariate logistic regression analysis. Variables that were predictive at the 0.1 level by using a univariate analysis were entered into the final multivariate analysis. A P-value less than 0.05 denoted statistical significance.
RESULTS
Over a 10-year interval, 8,327 patients underwent a colonoscopic polypectomy. Delayed postpolypectomy hemorrhage occurred in 92 patients (1.1%), who were selected as the case group. The average time between the procedure and bleeding was 2.71 ± 1.55 days. The control group consisted of 276 patients who had experienced an uneventful procedure. The baseline clinical characteristics of the case and the control groups were not significantly different (Table 1).
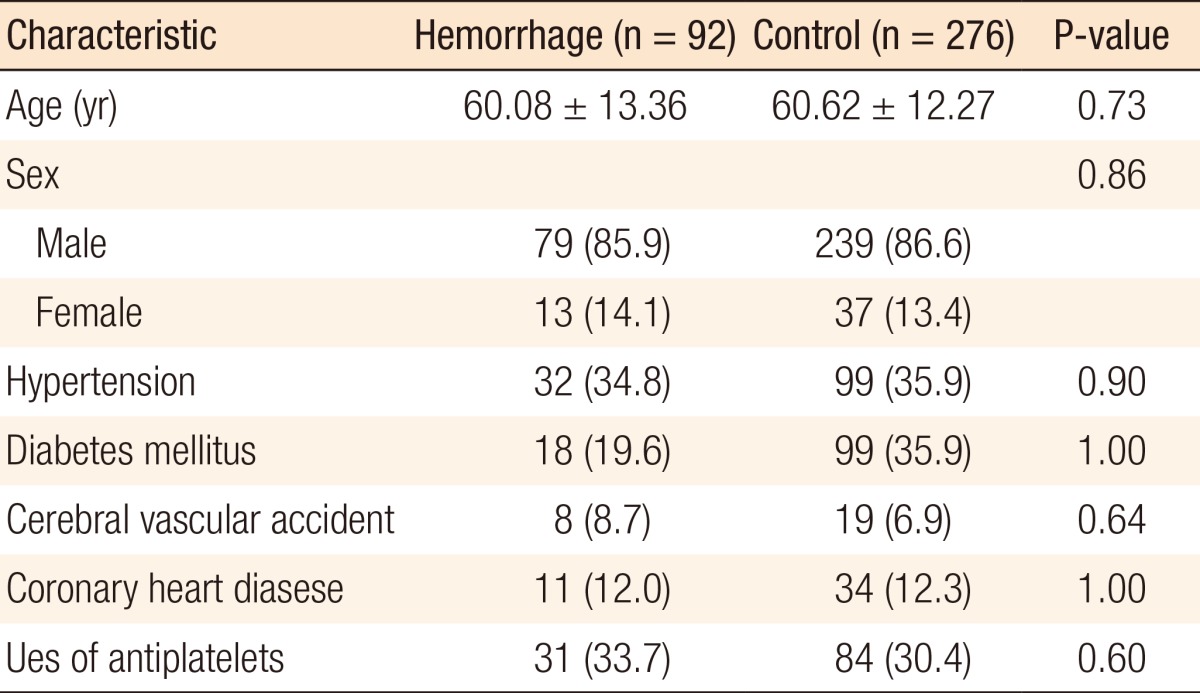
Basic characteristics and underlying condition-related risk factors for delayed postpolypectomy hemorrhage
Neither comorbidity nor use of antiplatelets had any significant association with delayed postpolypectomy hemorrhage (Table 1). No statistically significant difference was found between a snare polypectomy and an endoscopic mucosal resection in terms of inducing delayed postpolypectomy hemorrhage. The use of prophylactic hemostasis also showed no significant difference (Table 2).
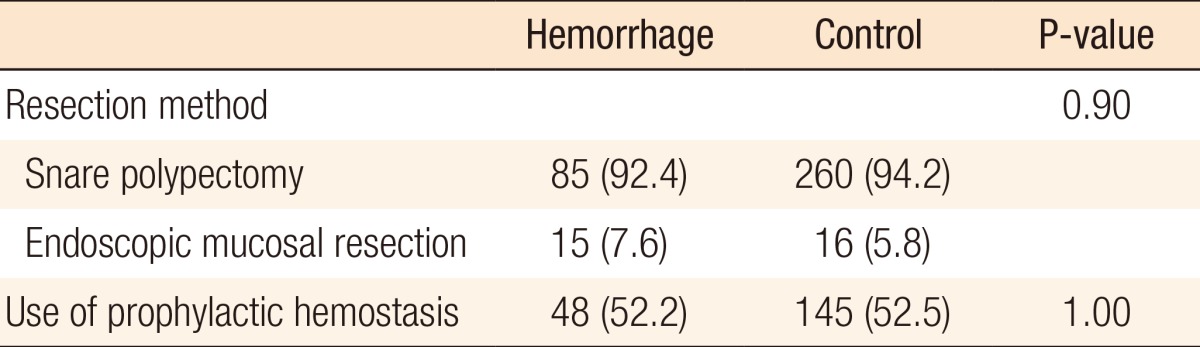
Procedure-related factors for delayed postpolypectomy hemorrhage
Both the univariate and the multivariate analyses showed that the size of the resected polyps was the only, and most important, predictor of delayed hemorrhage after a colonoscopic polypectomy (odds ratio [OR], 2.06; 95% confidence interval [CI], 1.12-1.27; P = 0.03). The average size of the resected polyps in the case group was 11.83 ± 4.47 mm, and in the control group, it was 10.70 ± 3.66 mm. The size of resected polyps was slightly larger in the case group than in the control group (P = 0.03). However, the multivariate analysis revealed that the risk of delayed bleeding increased by 24 percent for every 1 mm increase in the size of the resected polyp (OR, 1.24; 95% CI, 1.12-1.27; P = 0.03) (Tables 3, 4).
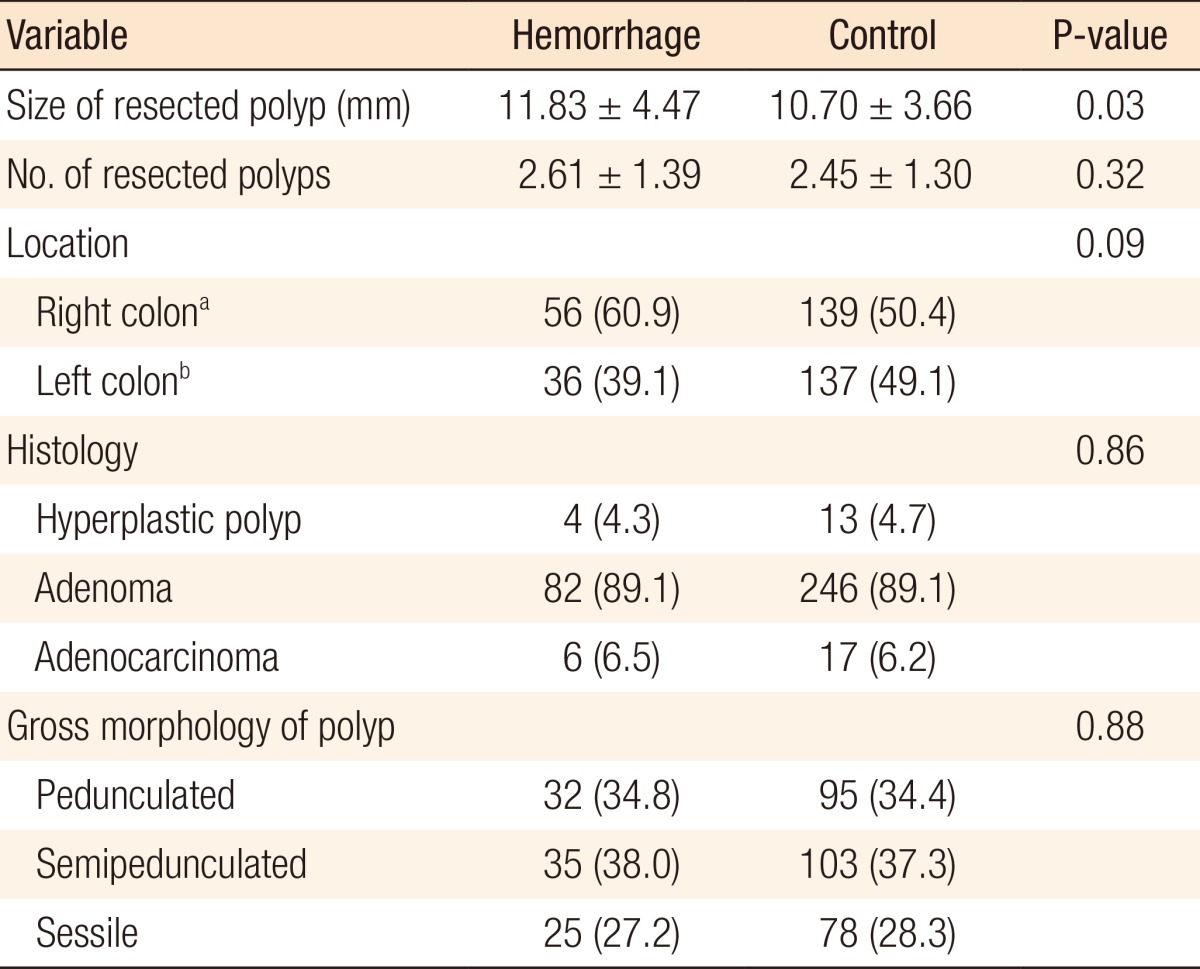
Polyp-related factors for delayed postpolypectomy hemorrhage

Multivariate analysis of risk factors for delayed postpolypectomy hemorrhage
DISCUSSION
A colonoscopic polypectomy is an effective tool for preventing colorectal cancer [1, 2, 3, 4]; however, it can induce several complications [5, 6]. The most commonly encountered complications of a polypectomy are hemorrhage and perforation [7, 8, 9, 10]. Postpolypectomy hemorrhage can be classified as immediate (defined as occurring during the procedure) or delayed (defined as occurring after the procedure) [6]. Approximately two-thirds of delayed hemorrhages stop spontaneously, although on rare occasions, some patients require a transfusion or further intensive treatment [5, 6, 7]. In Korea, in particular, many colonoscopic polypectomy procedures are performed on an out-patient basis, which means that delayed hemorrhage can occur outside the hospital, which raises concerns.
The risk factors for delayed postpolypectomy hemorrhage have been assessed by several studies [11, 12, 13, 14, 15]. For example, Watabe et al. [15] suggested that hypertension was a significant risk factor for delayed postpolypectomy hemorrhage. However, in our study, none of the comorbidities significantly affected the patient's related risk for delayed postpolypectomy hemorrhage.
The effect of antiplatelets use on postpolypectomy bleeding has been equivocal according to previous studies [16, 17]. Use of antiplatelets was not associated with delayed postpolypectomy hemorrhage in the present study. The American Society for Gastrointestinal Endoscopy [18] suggested that the use of a single antiplatelet agent should not be terminated prior to the polypectomy; our study would seem to support this recommendation.
In previous studies, polyp-related risk factors were significantly more important risk factors for postpolypectomy delayed hemorrhage than were either patient- or procedure-related risk factors [11, 12, 13, 14]. The size, number, location (right colon), and sessile form of the polyp were suggested as polyp-related risk factors [11, 12, 13, 14, 15]. Polyp size was determined in several previous studies to be the most reliable factor for predicting hemorrhage [11, 12, 14]. Similarly, in our study, the size of the resected polyps was the only independent risk factor for delayed bleeding, and the risk of delayed bleeding increased by 24% for every 1-mm increase in the resected polyp size (OR, 1.24; 95% CI, 1.12-1.27; P = 0.03).
Evaluation of procedure-related factors indicated no significant independent factor related to delayed postpolypectomy hemorrhage. Some studies have suggested that the endoscopist's experience can be an independent risk factor for delayed postpolypectomy hemorrhage [12, 13], but we included cases that had been performed by operators whose experience with a polypectomy was two or more years. Consequently, we did not analyze the endoscopist's experience as a risk factor. Some studies have suggested the use of argon plasma coagulation or endoclips for the prevention of postpolypectomy bleeding, but the effects of their use are still being debated [19,20,21,22]. Endoscopic mucosal resection, snare polypectomy, and use of prophylactic hemostasis had no significant effects on the risk of delayed hemorrhage in our study.
The number of subjects in the control group in our study was three times the number of subjects in the patient group, which helped in assessing highly-significant risk factors. However, our study also had some limitations. For example, it was conducted at a single center as a retrospective study based on medical records. Although we collected cases that were performed by surgeons who had two or more years' experience in the polypectomy procedure, our study could not reflect each endoscopist's skills, which may have had an influence on postpolypectomy complications, including delayed hemorrhage. We suggest that a large, multicenter, prospective study is needed to assess the risk factors for delayed postpolypectomy hemorrhage. We believe this would help in establishing effective guidelines for preventing this type of hemorrhage.
In conclusion, the size of the resected polyp is the only independent risk factor for delayed postpolypectomy hemorrhage. Surgeons who plan to perform a polypectomy of larger-sized polyps should keep the possibility of delayed hemorrhage in mind and should consider conducting a prophylactic hemostatic procedure before the polypectomy.
Notes
No potential conflict of interest relevant to this article was reported.