INTRODUCTION
An internal hernia occurs when viscera protrude through a congenital or acquired peritoneal or mesenteric aperture in the peritoneal cavity. Hernias account for 5.8% of intestinal obstruction cases [1,2,3]. Aperture types are paraduodenal (53%), pericecal (13%), foramen of Winslow (8%), transmesenteric and transmesocolic (8%), intersigmoid (6%), retroanastomotic (5%), and transomental (1%ŌĆō4%) [4]. Transomental hernias are very rare and usually congenital; they are rarely traumatic or iatrogenic [5,8,7]. We report a case of a spontaneous transomental hernia of the small intestine causing intestinal obstruction.
CASE REPORT
A 57-year-old man was admitted to the Emergency Department with an acute abdomen. He reported abrupt onset of epigastric pain and bilious vomiting with abdominal distension for at least the preceding 24 hours. The patient could not recall previous, similar pain attacks. He had no prior surgical procedures or history of abdominal trauma.
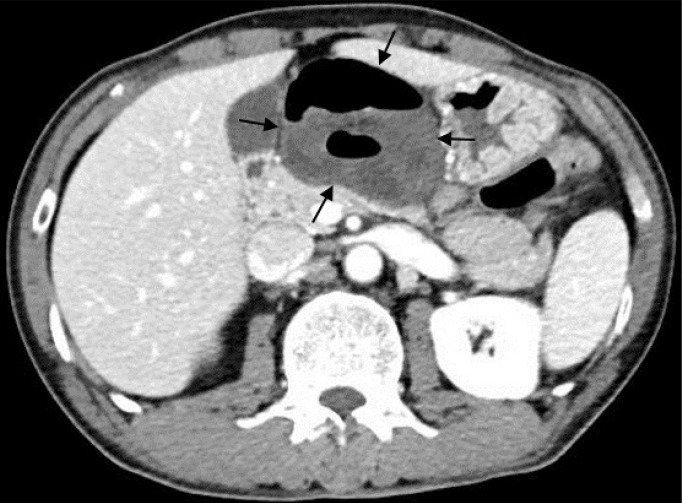
Vital signs were all within normal limits. On physical examination, the abdomen was mildly distended and tympanic on percussion. The abdomen showed epigastric tenderness, but not rebound tenderness, and had audible hyperactive bowel sounds. The patient had no visible abdominal surgical scars. Laboratory tests were unremarkable except for leukocytosis (14.09 ├Ś 103 /mL with 88.8% neutrophils). A plain film of the abdomen demonstrated dilated small bowel loops with an air-fluid level in the epigastrium and on the right side of the abdomen, suggesting intestinal obstruction (Fig. 1). A computed tomography (CT) scan of the abdomen revealed dilated, hypo-enhancing small bowel loops with a swirling pattern in the mesenteric vessels surrounded to the right by the gallbladder and liver, to the left by the stomach, and posteriorly by the pancreas (Figs. 2, 3). An internal hernia with strangulation of the small bowel in the lesser sac was suspected.
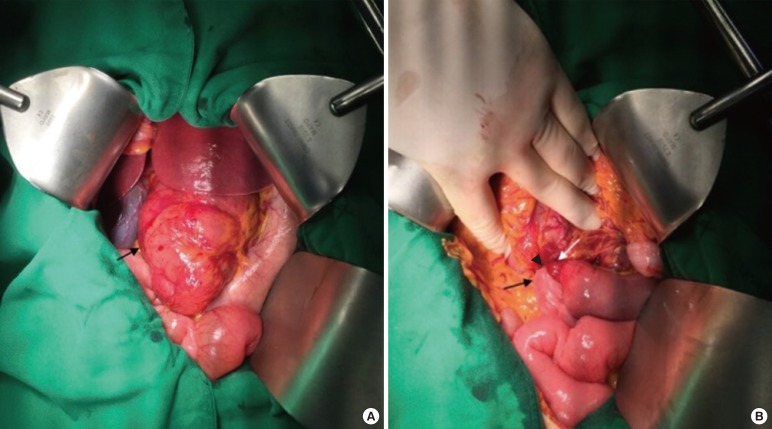
An emergency laparotomy was performed. An approximately 50-cm segment of the jejunum and the proximal ileum in the lesser sac was herniated through a 2.0-cm slit-like defect in the distal part of the gastrocolic ligament (Fig. 4A, B). The incarcerated small bowel loops appeared congested, but did not strangulate. After reduction of small bowel loops, the ischemic signs of the herniated loops recovered. The omentum was divided. The postoperative course was uneventful. The patient was discharged on the ninth day after entering the hospital.
DISCUSSION
Internal hernias are protrusions of the viscera through a peritoneal or mesenteric opening, with the herniated viscera remaining within the abdominal cavity. Openings have normal (foramen of Winslow), paranormal (paraduodenal, ileocecal, supravesical fossa), and abnormal (transomental defect) anatomies [1,8]. Based on autopsy studies, the overall incidence of internal hernias is 0.2%ŌĆō0.9% [1]. Internal hernias constitute up to 0.6%ŌĆō5.8% of all intestinal obstructions [2,9]. Hernia mortality may exceed 45% [2,9].
A transomental hernia through the greater or lesser omentum is rare, accounting for approximately 1%ŌĆō4% of internal hernias [1]. Transomental hernias are generally reported in patients aged over fifty [10]. In such instances, acquired transomental hernias are usual, are commonly iatrogenic, and result from surgical interventions (Roux-end-Y gastric bypass, liver transplantation, and small bowel or colon resection) or from trauma or peritoneal inflammation [5,8,7]. In children, congenital transomental hernias are common and occur in males versus females at a ratio of about 2 to 1 [6]. In children, disease severity depends on the orifice size and the length of the herniated small bowel loops [11]. In rare cases, such as the one described in this study, internal hernias through the greater or lesser omentum occur spontaneously as the result of senile atrophy without history of surgery, trauma, or inflammation [10]. Yamaguchi [12] classified transomental hernias as type A (peritoneal cavity ŌåÆ greater omentum ŌåÆ peritoneal cavity), B(peritoneal cavity ŌåÆ omental bursa ŌåÆ peritoneal cavity), or C (peritoneal cavity ŌåÆ omental bursa). Type A is slightly more common than type C, and type A is predominant in older patients [12]. Our case was type C.
Transomental hernias are difficult to diagnosis. Clinical manifestations are not specific and are similar to acute obstructive syndrome including nausea, vomiting, abdominal pain, distended abdomen, and constipation. Compared with other types of internal hernias, patients with transomental hernias present more frequently with strangulation of the small bowel. In most cases, a gangrenous bowel is present at the exploratory laparotomy [9]. For this reason, transomental hernias have a high postoperative mortality rate of 30%, so emergency diagnosis and treatment are critical [6,9].
Abdominal CT scans are helpful for diagnosis. Abdominal CT scans may reveal dilated small bowel loops with a "beak sign," which is a triangular configuration of the transition zone between the proximal dilated bowels and the herniated bowel segments or between dilated, herniated bowel segments and distal, collapsed bowel segments [7]. CT might also reveal a swirling pattern of the mesenteric vessels, engorged mesenteric vessels with a large impact on the surrounding organs and bowel wall thickening [13]. In addition, a transomental hernia should be suspected if the dilated small bowel loops are localized in the lesser sac (i.e., surrounded to the right by the gallbladder and liver, to the left by the stomach, and posteriorly by the pancreas) and the neck of the hernia orifice is seen as mesenteric vessels passing through the omental defect, with abdominal CT scans showing no evidence of loops passing through the foramen of Winslow between the inferior vena cava and the portal triad [14]. However, in most cases, a definitive diagnosis is established intraoperatively [14].
Surgical treatment is the reduction of the herniated intestinal segments. If necrosis, perforation, or irreversible ischemia of the herniated viscera is present, bowel resection is necessary. In sequence, the defect of omentum must be repaired to prevent subsequent herniation. Even without risk factors of previous abdominal surgery, trauma or peritoneal inflammation, the possibility of small bowel obstruction secondary to the internal hernia should be considered. Surgical treatment based on high clinical suspicion can reduce the risk of complications and postoperative mortality in patients with a transomental hernia.