INTRODUCTION
In 2012, 28,988 individuals in Korea were newly diagnosed with colorectal cancer. Colorectal cancer has become the second most common cancer in Korean men and the third most common in Korean women, and its incidence has continued to increase in both sexes [1]. Colonoscopy has become the gold standard screening test for colorectal cancer. Because a colonic adenoma is related to interval cancer [2], colonoscopic removal of adenomatous polyps reduces the incidence of and the mortality from colorectal cancer [3,4,5]. The U.S. Multi-Society Task Force on Colorectal Cancer has targeted the adenoma detection rate for quality improvement during colonoscopy [6], with the adenoma detection rate being regarded as an important indicator of the quality of colonoscopy [7,8,9].
The diagnostic accuracy and the therapeutic safety of screening colonoscopy depend on the quality of bowel preparation. Adequate bowel preparation is essential for a successful inspection of the colonic mucosa [10,11,12]. Little is known about the impact of the quality of bowel preparation on the adenoma detection rate during screening colonoscopy. This study was, therefore, designed both to evaluate the association between the adenoma detection rate and the quality of bowel preparation and to assess the risk factors associated with adenoma detection.
METHODS
Study population
The medical charts of 1,079 individuals who had undergone screening colonoscopies at the National Cancer Center in Korea between December 2012 and April 2014 were retrospectively reviewed. Subjects with inadequate bowel preparations (n = 47, 4.4%) were excluded because additional bowel preparation was needed. Thus, colonoscopies of 1,032 individuals were included in the analysis. Each started bowel preparation with PEG-3350 plus ascorbic acid (Coolprep, Taejoon, Seoul, Korea) between 6:00 PM and 10:00 PM on the evening before the colonoscopy. Colonoscopies were performed between 9:00 AM and 12:00 noon. This study was approved by the Institutional Review Board of National Cancer Center (NCC2014-0132).
Definitions
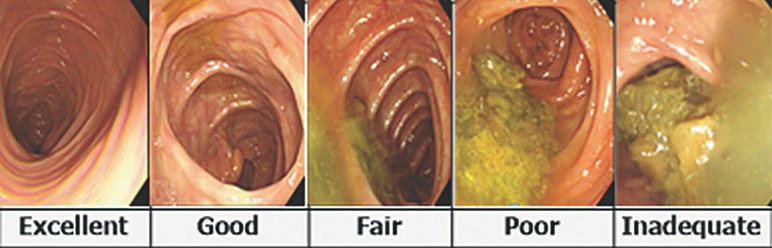
Bowel preparations were classified by using the Aronchick scale (Fig. 1) based on the proportion of fluid and remnant stool [13]. Excellent was defined as the presence of a small volume of clear liquid or visualization of greater than 95% of the surface, good as a large volume of clear liquid covering 5% to 25% of the surface but visualization of greater than 90% of the surface, fair as the presence of some semisolid stool that could be suctioned or washed away but visualization of greater than 90% of the surface, poor as the presence of semisolid stool that could not be suctioned or washed away and visualization of less than 90% of the surface, and inadequate as solid stool that impeded visualization, requiring repeat preparation and colonoscopy.
The adenoma and the polyp detection rates were defined as the proportion of subjects with at least one adenoma or polyp divided by the total number of colonoscopies. Advanced adenomas are typically defined as adenomas greater than or equal to 1 cm in diameter or those with villous components (tubulovillous or villous) or with high-grade or severe dysplasia [14].
Statistical analysis
Continuous variables were compared using the Student t-test whereas categorical variables were compared using the chi-square or Fisher exact test. Logistic regression was used for multivariate analyses to determine the independent risk factors for adenoma detection. An analysis of variance was used to compare the quality of colonoscopy between bowel preparation groups. A P-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using the SPSS ver. 14.0 ( SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
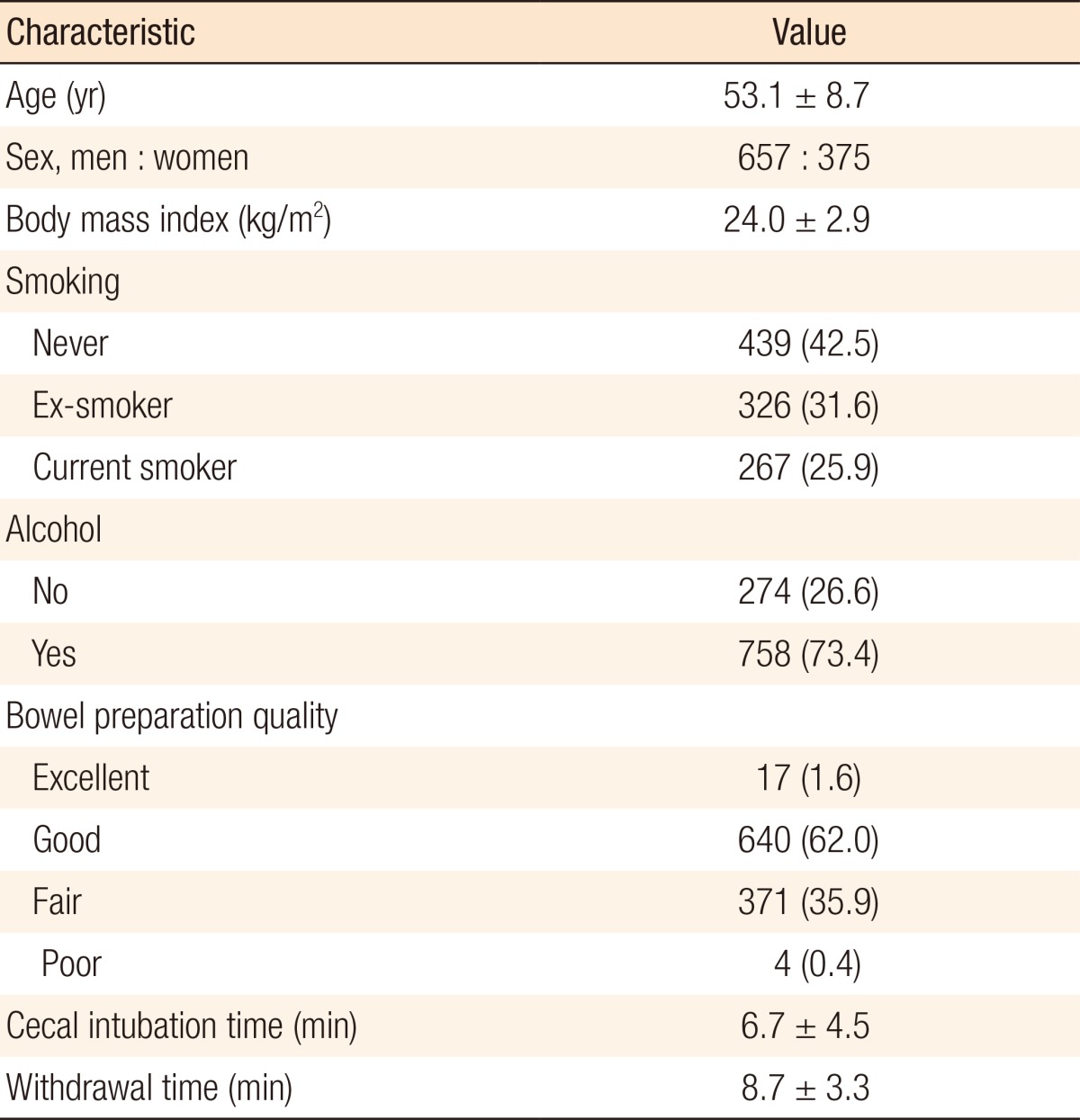
The baseline characteristics of the 1,032 individuals included in this study are shown in Table 1. The mean age of these subjects was 53.1 years; 657 (63.7%) were men and 375 (36.3%) were women. The mean body mass index was 24.0 kg/m2. The mean cecal intubation time was 6.7 minutes, and the mean withdrawal time was 8.7 minutes. Bowel preparation was excellent, good, fair, and poor in 17 (1.6%), 640 (62.0%), 371 (35.9%), and 4 subjects (0.4%), respectively.
Bowel preparation and quality of colonoscopy
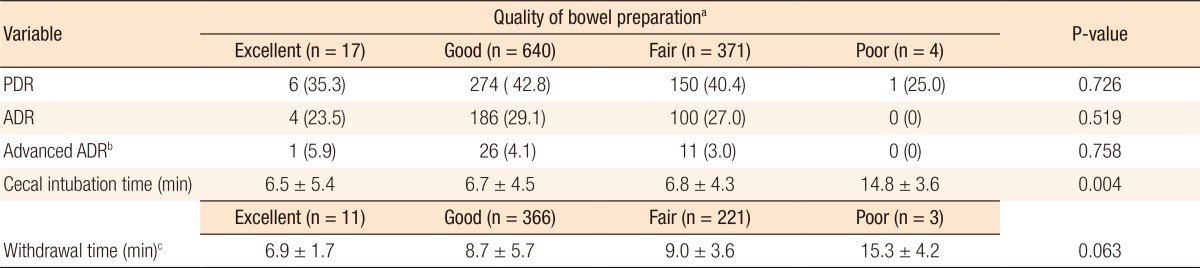
The overall rates of adenoma, polyp, and advanced adenoma detection were 28.1%, 41.8%, and 3.7%, respectively. The adenoma detection rate was 31.8% in men and 21.6% in women. The polyp detection rates in subjects who underwent excellent, good, fair, and poor bowel preparation were 35.3%, 42.8%, 40.4%, and 25.0%, respectively (P = 0.726). The adenoma detection rates in these groups were 23.5%, 29.1%, 27.0%, and 0%, respectively (P = 0.519), and the advanced adenoma detection rates were 5.9%, 4.1%, 3.0%, and 0%, respectively (P = 0.758). The cecal intubation time was significantly affected by bowel preparation (P = 0.004), being longer in subjects with poor bowel preparation. In contrast, withdrawal time was not significantly associated with the quality of bowel preparation (P = 0.063) (Table 2).
Risk factors for the adenoma detection rate
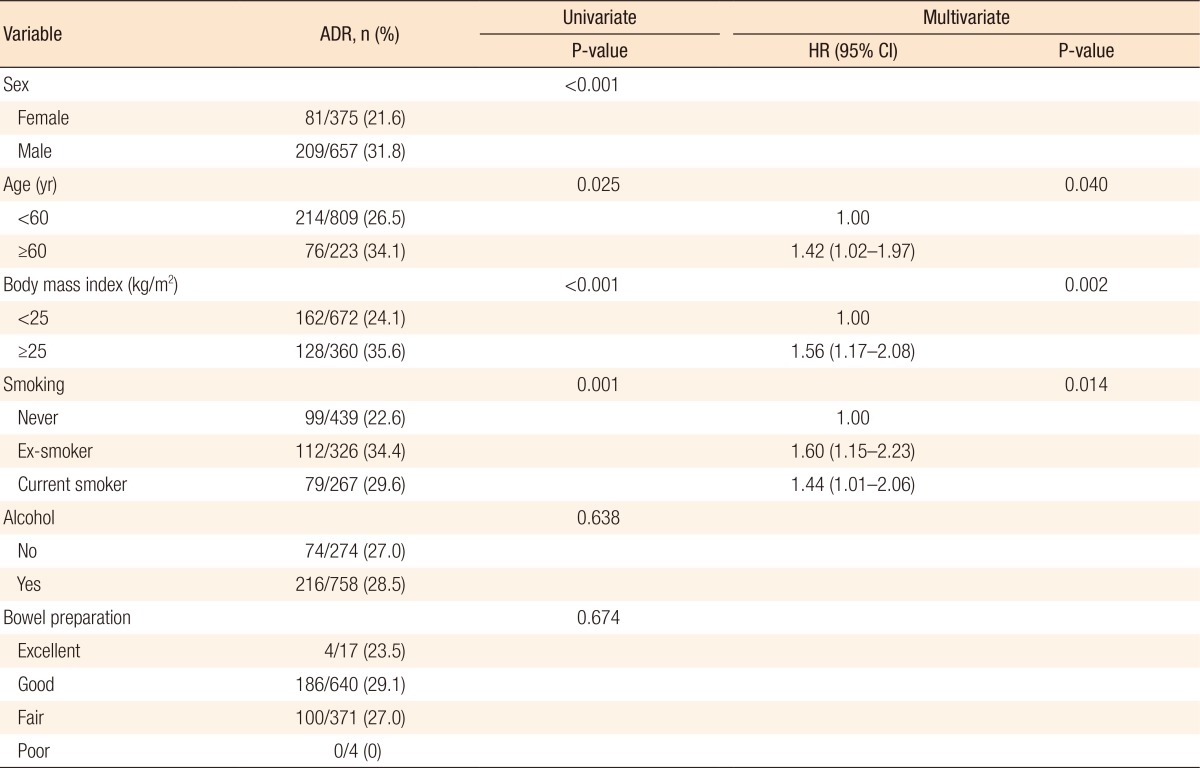
Table 3 shows the results of the univariate and the multivariate analyses of the risk factors for adenoma detection. The univariate analysis showed that male sex, age ≥ 60 years, body mass index (BMI) ≥ 25 kg/m2, and current smoking were significant risk factors for adenoma detection. The multivariate analysis showed that age ≥ 60 years (hazard ratio [HR], 1.42; 95% confidence interval [CI], 1.02–1.97; P = 0.040), BMI ≥ 25 kg/m2 (HR, 1.56; 95% CI, 1.17–2.08; P = 0.002) and current smoking (HR, 1.44; 95% CI, 1.01–2.06; P = 0.014) were independent risk factors for adenoma detection.
DISCUSSION
Previous studies assessing the relationship between the adenoma detection rate and bowel preparation have yielded various outcomes. For example, one study reported that the adenoma detection rate for good bowel preparation was significantly higher than it was for excellent bowel preparation [15] whereas another study found no significant difference between good and excellent bowel preparation [16]. Other studies found that the adenoma detection rate was not significantly different in subjects with fair bowel preparation compared to those with excellent and good bowel preparation [17,18], although the rate of missed adenomas after poor bowel preparation was significantly higher than it was after excellent, good or fair bowel preparation [19]. In contrast, adenoma detection rates were reported to be similar after excellent (24.2%), good (26.8%), fair (32.1%), and poor (22.1%) bowel preparation [20]. Similarly, this study found that adenoma detection rates were unrelated to the degree of bowel preparation. As the rate of poor bowel preparation (n = 4, 0.4%) was very low, this subgroup was excluded from comparative analyses. Nevertheless, a comparison of three groups of subjects, those with excellent, good, and fair bowel preparation, showed no significant differences in the polyp (P = 0.654), the adenoma (P = 0.704), and the advanced adenoma (P = 0.599) detection rates.
Bowel preparation was found to be inadequate in 47 subjects, with adenomas detected in 12 of these subjects (25.5%). Because all subjects with inadequate bowel preparation required repeat bowel preparations, actual bowel preparation grades were changed following the repeat colonoscopies. Overall, these findings suggest that the incidences of colorectal adenomas were similar in subjects with adequate preparation and those with inadequate bowel preparation.
This study also found that age ≥ 60 years, BMI ≥ 25 kg/m2, and smoking were independent risk factors for adenoma detection. Similarly, age over 50 years was found to be associated with a high adenoma detection rate [21], and a multivariate meta-analysis confirmed a positive association between higher BMI and the prevalence of colorectal adenomas [22]. Other studies found that cigarette smoking [23] and male sex [24] were independently associated with a higher adenoma detection rate. Although our study found that the adenoma detection rate was higher in men than in women, the multivariate analysis demonstrated that sex was not an independent risk factor for adenoma detection (P = 0.240).
Characteristics associated with the adenoma detection rate during screening colonoscopy can be classified as patient factors, colonoscopist factors, and endoscope factors [25]. Patient-associated factors include male sex, age, BMI ≥ 25 kg/m2, familial and personal history of colorectal polyps and colorectal cancer, positive fecal occult blood test results, cigarette smoking, alcohol consumption,
and bowel preparation [21,22,23,24,25]. Colonoscopist-associated factors include the cecal intubation time, the withdrawal time, the colonoscopist's training and experience, the use of intravenous antispasmodics, and the procedure start time [26,27,28]. Endoscope factors include the generation of the instrument used [25]. The risk factors for colorectal adenoma detection, including older age, being overweight, male sex, and smoking, are also risk factors for colorectal adenomas [23,29].
The rates of detection of any neoplasia and of advanced neoplasia have been reported to be higher in subjects with mean withdrawal times longer than or equal to 6 minutes than in those with withdrawn times shorter than 6 minutes [27]. The mean withdrawal time of our study subjects was 8.7 minutes, with both the cecal intubation time and the withdrawal time being longer in subjects with poor bowel preparation. These longer times are likely due to poor visualization during colonoscope insertion, suggesting that suction and irrigation may improve visualization of the colonic mucosa during instrument withdrawal. The cecal intubation time (P = 0.863) and the withdrawal time (P = 0.359), however, were similar in subjects with excellent, good, and fair bowel preparation.
The adenoma detection rates during screening colonoscopy have been reported to range from 9.4% to 37.5% [30]. The overall adenoma detection rate among subjects in this study was 28.1%. The American Society of Gastrointestinal Endoscopy and the American College of Gastroenterology Task Force recommended minimal adenoma detection rates of more than 25% for average-risk men aged 50 years or older and of more than 15% for average-risk women aged 50 years or older [6,8]. The adenoma detection rates of men and women in this study were even higher, being 31.8% and 21.6%, respectively.
This study had several limitations. First, it was retrospective in design and involved individuals at a single institution. Second, the sample sizes of the four bowel preparation groups were uneven, with few subjects in the poor bowel preparation group, suggesting that this group may have had an outsized effect on our study results. Third, because this study did not include all possible risk factors associated with adenoma detection, the results of this study may not be generalizable.
In conclusion, the adenoma detection rate was unrelated to the quality of bowel preparation for screening colonoscopy. Independent risk factors for the adenoma detection rate included older age, obesity, and smoking.