Colorectal Cancer with Multiple Metastases: Is Palliative Surgery Needed?
Article information
Abstract
In patients with symptomatic incurable metastatic colorectal cancer (mCRC), the goal of resection of the primary lesion is to palliate cancer-related morbidity, including obstruction, bleeding, or perforation. In patients with asymptomatic primary tumors and incurable metastatic disease, however, the necessity of primary tumor resection is less clear. Although several retrospective analyses suggest survival benefit in patients who undergo resection of the primary tumor, applying this older evidence to modern patients is out of date for several reasons. Modern chemotherapy regimens incorporating the novel cytotoxic agents oxaliplatin and irinotecan, as well as the target agents bevacizumab and cetuximab, have improved median survival from less than 1 year with the only available single-agent 5-fluorouracil until the mid-1990s to over 2 years. In addition to significant prolongation of overall survival, combinations of novel chemotherapeutic and target agents have allowed improved local and distant tumor control, decreasing the likelihood of local tumor-related complications requiring surgical resection. Resection of an asymptomatic primary tumor risks surgical complications and may postpone the administration of chemotherapy that may offer both systemic and local control. In conclusion, the morbidity and the mortality of unnecessary surgery or surgery that does not improve quality of life or survival in patients with mCRC of a limited life expectancy should be carefully evaluated. With the availability of effective combinations of chemotherapy and target agents, systemic therapy for the treatment of life-threatening metastases would be a preferable treatment strategy for unresectable asymptomatic patients with mCRC.
INTRODUCTION
According to the 2010 cancer statistics from the Ministry of Health and Welfare, Korea, colorectal cancer (CRC) in 2008 accounted for 12.7% (22,623 cases) of all cancers and was reported to be third leading primary type of cancer after stomach and thyroid cancer (second after stomach cancer in men, and fourth after thyroid, breast and stomach cancer in women) [1]. About 20-25% of patients with CRC are known to present with metastases at the time of initial diagnosis [2]. Therefore, appropriate management of patients with metastatic CRC (mCRC) is an important oncologic issue.
Recent advancements in combination chemotherapy and target agents for CRC have increased the survival of incurable mCRC remarkably compared with that in the 1990s when 5-fluorouracil (5-FU) was the only available active agent [3]. Nonetheless, less than 10% of patients with mCRC are alive at 5 years, with most patients dying from their cancer [4]. In mCRC, a palliative surgical resection of the primary tumor can be performed to prevent tumor-related complications, such as obstruction, bleeding and perforation, and thus to minimize cancer-related morbidities. In selected patients, long-term survival can be expected when both the primary and all metastatic diseases are ressected. However, resection of the primary tumor in patients with mCRC is associated with 1-6% of surgical mortality and 20-30% of postoperative morbidity [5-9]. Therefore, potential morbidities and adverse impacts on quality of life associated with treatment, as well as survival benefit, should be considered seriously when treating patients with mCRC, for whom a limited life expectancy is predicted.
No standard treatment guidelines have yet been established for primary treatment of patients with asymptomatic primary tumors and incurable metastatic disease. In these circumstances, two treatment strategies can be considered. First, as in patients with symptomatic primary tumors and incurable metastatic disease, resection of asymptomatic primary tumors can be performed to prevent later tumor-associated complications. Second, primary chemotherapy using novel agents can be tried without surgical resection. Here, evidence supproting palliative primary tumor resection in incurable mCRC was critically reviewed and compared with evidence supporting chemotherapy using novel cytotoxic and target agents.
RETROSPECTIVE ANALYSES OF AND RESPONSE TO CHEMOTHERAPY
To date, no prospective randomized studies exist to guide standard treatment in patients with incurable mCRC. Considering treatment of these patients with a limited life expectancy, such issues as survival benefit of a treatment option, treatment-related complications (including morbidity and mortality), and their impact on quality of life should be weighed. The ultimate goal of treating unresectable mCRC should be palliative and be focused on prolongation of survival and maintenance of quality of life.
In patients with symptomatic primary tumors and unresectable metastatic disease, palliative resection of the symptomatic primary tumor is often required because of cancer-related complications, such as obstruction, intractable bleeding, and perforation. Although surgical resection can palliate symptoms associated with primary lesions effectively, a serious consideration should be paid to surgical complications and mortality. As previously mentioned in the introduction, morbidity and mortality associated with palliative resection cannot be ignored [5-9]. Surgical problems associated with palliative resection of colorectal primary should be considered seriously, in particular, in patients with asymptomatic incurable mCRC. There is no level I evidence for selected treatment (primary colorectal resection or primary chemotherapy) of patients with asymptomatic unresectable mCRC. No prospective randomized trials concerning this issue exist. Although some non-randomized, retrospective reviews suggest a gain in survival from resection of the asymptomatic primary tumors [6, 9-11], this survival benefit was thought to reflect selection bias; that is, patients were not randomly selected at all, and patients selected for surgery tended to be those with lower tumor burden, higher performance status, and younger age. Therefore, comparing the survival of those patients with patients who had undergone primary chemotherapy seems to be of no value. Moreover, The most commonly used chemotherapeutic agent in those retrospective studies was 5-FU, which could not prolong median survival by even a year, far less than the survival benefits offered from the combination regimens currently available. Recently, novel cytotoxic agents, such as oxaliplatin and irinotecan, and target agents, such as bevacizumab (monoclonal antibody for vascular endothelial growth factor) and cetuximab (monoclonal antibody for epidermal growth factor receptor), have been developed and are now widely being used for treatment of unresectable mCRC, whereby the median survival of less than a year achieved by using single 5-FU has been increased to over two years in recent years [3]. Table 1 summarizes the outcomes of several major trials that define the standard of care using modern chemotherapy in mCRC [12-16].
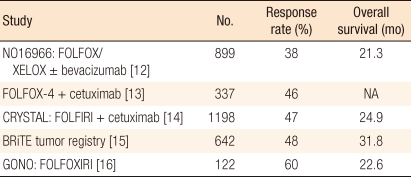
Novel chemotherapy regimens for colorectal cancer
SELECTION OF TREATMENT IN PATENTS WITH ASYMPTOMATIC UNRESECTABLE MCRC
To date, medical evidence for the selection of treatment for asymptomatic unresectable/incurable mCRC is still insufficient, and it would be important to consider the following several factors in the determination of a proper option:
Response of the primary colorectal tumor to chemotherapy
In mCRC, oncologic assessments of chemotherapy currently available are primarily focused on the presence or absence of response to metastatic lesions. If this is the case and primary chemotherapy without surgery of the primary tumor is planned in patients with unresectable asymptomatic mCRC, whether the primary tumor, as well as metastatic lesions, is responsive to chemotherapy or not must be considered. Chau et al. [17] analyzed a phase II study evaluating the effect of neoadjuvant chemotherapy on 77 patients with poor-risk rectal cancer. Patients received 12 weeks of capecitabine and oxaliplatin (XELOX regimen) prior to neoadjuvant chemoradiotherapy using capecitabine. Based on an assessment of evidence of rectal bleeding, pelvic pain, tenesmus, diarrhea, and constipation, the objective response rate after 12 weeks of neoadjuvant XELOX was 88%, and 86% of the patients with symptoms improved. Specifically, pelvic pain/tenesmus was decreased in 71% of the patients, 90% had improvement in diarrhea/constipation, and 100% had reduced rectal bleeding (Table 2) [17]. These results suggest that the response of the primary tumor to chemotherapy is, at least, equivalent to that of metastatic lesions and that primary chemotherapy without surgery can be a preferred treatment strategy in patients with asymptomatic unresectable mCRC.

Symptomatic improvement after neoadjuvant chemotherapy
The response rate of primary chemotherapy in mCRC using 5-FU/leucovorin used to be about 20%; however, combinations of infusional 5-FU/leucovorin with oxaliplatin (FOLFOX) or irinotecan (FOLFIRI) have yielded response rates of 50% [18, 19]. Furthermore, the addition of a target agent, bevacizumab or cetuximab, to the above combinations has provided clinically meaningful improvement in response rate and survival for these patents [13, 14, 20, 21]. When target agents are used, toxicity associated with administration needs to be kept in mind. For example, bevacizumab has been associated with a 1% to 2% incidence of gastrointestinal perforation, and the risk of perforation at the site of the primary tumor is increased when the agent is administered in patients with unresectable mCRC with the primary tumor in situ [22]. When considering the administration of cetuximab, the KRAS mutation status of tumors should be examined because survival benefit is seen mainly in patients with wild type KRAS [13, 14].
Risk of complications in the primary tumor
When planning primary chemotherapy without surgery in patients with asymptomatic unresectable mCRC, the risk of primary tumor-related complications (e.g., obstruction, bleeding and perforation), which require operative or nonoperative intervention, during treatment can be considered as a second factor. In other words, when performing primary chemotherapy while leaving the primary tumor intact, the concern is whether the risk of developing primary tumor-related complications during chemotherapy would be significantly higher as compared to when the primary tumor is surgically resected. A clear conclusion about this issue can be attained from the evidence analyzed by Poultsides et al. [23]. They analyzed the frequency of interventions necessary to palliate the intact primary tumor in patients who present with synchronous, stage IV CRC and who receive up-front modern combined chemotherapy (FOLFOX, IFL, FOLFIRI/±bevacizumab) without prophylactic surgery. Of 233 patients, 207 (89%) never required surgical palliation of their primary tumor. Sixteen patients (7%) required emergent surgery for primary tumor obstruction or perforation, and 10 patients (4%) required nonoperative intervention, such as stent or radiotherapy (Fig. 1) [23]. Tebbutt et al. [24] also compared the incidence of major intestinal complications in patients who received chemotherapy treatment with or without prior palliative resection of the primary tumor. Intestinal obstruction affected 13.4% of the patients in the unresected group and 13.2% of the patients in the resected group (P = 0.96). The incidences of peritonitis, fistula formation, and intestinal hemorrhage in the unresected group were not significantly different from those in the resected group, either. Such evidence suggests that chemotherapy may be successfully used as an initial treatment for patients who have not undergone an initial resection of the primary tumor with no increased risk of most major intestinal complications compared with patients who have undergone an initial resection of the primary tumor. Moreover, palliative resection of an asymptomatic primary tumor may unnecessarily subject patients to surgery-related complications, and these potential surgical complications may postpone the administration of chemotherapy, which may offer better survival benefit.

Outcomes of unresected primary tumors in 233 patients with synchronous stage IV colorectal cancer who received modern combination chemotherapy. Curative resections, combined resections of colorectal tumor and metastatic disease, were elective. Preemptive resections were performed in asymptomatic patients undergoing hepatic artery infusion pump placement. EBRT, external-beam radiation therapy for rectal cancer palliation.
Recently, nonoperative interventions have widely used to treat obstruction or bleeding from primary colorectal tumors. A self-expanding metallic stent (SEMS) by an endoscopic or an interventional radiologic approach can restore bowel patency effectively in many patients with malignant colon or rectal obstruction. Camunez et al. [25] reported excellent results of SEMS in the treatment of malignant colorectal obstruction: stent placement was successful in 70 of the 80 patients and resolved bowel obstruction in 67 patients (96%). In addition, more than 90% of stents remained patent for 6 months or more following placement. Clinically significant bleeding is present in about 10% of patients with mCRC [3], and although not commonly practiced in Korea, endoscopic laser therapy, cryotherapy, radiation therapy, and photodynamic therapy may be effective in controlling bleeding [26, 27]. Pelvic or perineal pain secondary to local invasion in patients with locally advanced rectal cancer can be alleviated effectively by radiotherapy.
Recent evidences support primary chemotherapy without prophylactic resection of the primary tumor in patients with asymptomatic mCRC does not increasing the risk of most tumor-associated intestinal complications compared with patients who have undergone an initial resection of the primary tumor. Thus, this approach, chemotherapy without resection, can be used as the standard practice in patients with asymptomatic primary colorectal tumors and unresectable metastatic diseases.
Survival rate
Several retrospective analyses report survival benefit from resection of the primary tumor; the median survival ranged from 14 to 23 months, which is more favorable than the 8.2 to 22 months in patients with chemotherapy as the first treatment [5, 6, 24, 26, 28, 29]. Although Tebbutt et al. [24] described a median survival of 8.2 months in the group initially treated with chemotherapy compared with 14 months in the group initially treated with resection, a multivariate analysis revealed that performance status and the presence of peritoneal or omental metastases were significant factors affecting survival and that resection status of the primary tumor was not significantly associated with survival. The study of Ruo et al. [6] also showed a survival benefit in the resection group (16 vs. 9 months), but resection status was not significantly associated with survival from a univariate analysis. Another point to consider would be the chemotherapeutic agent administered. Most retrospective analyses reflect systemic chemotherapy using a single agent, 5-FU, prior to the availability of oxaliplatin, irinotecan, bevacizumab, and cetuximab. As mentioned earlier, recent novel cytotoxic agents and target agents have increased survival to over two years in patients with unresectable mCRC. Considering these survival benefits obtained by administering modern chemotherapeutic regimens, no further survival benefit can be obtained by resection of the primary tumor in patients with asymptomatic unresectable mCRC. In this sense, it is desirable to carry out initial primary chemotherapy using the novel cytotoxic and target agents in patients with asymptomatic unresectable mCRC. The National Comprehensive Cancer Network (NCCN) guideline, 2011 also recommends initial chemotherapy using various novel agents for the primary treatment for non-obstructive unresectable mCRC [30].
CONCLUSION
For patients with incurable mCRC, resection of the asymptomatic primary tumor provides little palliative benefit, can give rise to major morbidity and mortality, and may potentially postpone the administration of systemic chemotherapy of high response. In patients with unresectable mCRC, initial resection of the primary tumor should only be performed after careful consideration and should be reserved for patients who may develop primary tumor-specific complications. With the availability of effective novel agents, systemic chemotherapy should be the preferred treatment strategy for unresectable asymptomatic patients with mCRC.
Notes
No potential conflict of interest relevant to this article was reported.