Pneumatic Colorectal Injury Caused by High Pressure Compressed Air
Article information

Abstract
The pneumatic colorectal injury caused by high pressure compressed air are rare and can be fatal. Herein, we present a case of 45-year-old male who developed sudden onset of severe abdominal pain after cleaning the dust on his pants with high pressure compressed air gun dust cleaner. Emergent exploratory laparotomy was done which findings are a huge rectal perforation with multiple serosal and subserosal tear in sigmoid to splenic flexure of colon. Anterior resection with left hemicolectomy, and temporary transverse colostomy was performed. Postoperative course was uneventful. Recently, prognosis is generally favorable because of prompt diagnosis and emergent surgical management.
INTRODUCTION
Because the use of high pressure compressed air has increased in many work places, the risk of associated pneumatic injuries is also increasing. Most pneumatic colorectal injuries usually occur when the air hose is directly inserted into the anus as a practical joke [1]. However, pneumatic colorectal injury can occur without inserting the air hose into the anus, and the perineal blasting with high pressure compressed air can penetrate barriers such as clothes and the anal sphincter, which can cause colorectal injuries either with or without perforation [1, 2]. We present the case of a 45-year-old male who developed sudden onset of severe abdominal pain after cleaning the dust on his pants with a high pressure compressed air gun dust cleaner.
CASE REPORT
This study was approved by the Institutional Review Board (IRB) of Chungbuk National University Hospital and informed consent was waived by the IRB. A 45-year-old male who developed sudden onset of severe abdominal pain was admitted to the emergency department. A few hours previously, he reported that he had cleaned the dust on his pants with a high pressure compressed air gun, and his friends placed the air nozzle too close to his buttocks as a practical joke. The patient had severe lower abdominal pain that progressed to the whole abdomen, and had abdominal distension and hematochezia. On physical examination, the abdomen was markedly distended, with generalized tenderness and rebound tenderness. The erect chest X-rays (Fig. 1) showed a marked presence of pneumoperitoneum and transverse colon dilatation. A small amount of bloody stool gushed out, on digital rectal examination. He was hemodynamically stable with a blood pressure of 150/70 mmHg, heart rate of 84 beats/min, respiratory rate of 28 breaths/min and body temperature of 35.5°C. Laboratory tests showed mild leukocytosis which was seen as a white blood cell count 11.13 × 103 /μL, and otherwise showed no specific findings. On abdominal and pelvic computed tomography (APCT), a focal wall defect was seen at the rectum with abundant fecal material in the pelvic cavity (Fig. 2A), and multiple subserosal pneumotosis was seen from the descending to distal transverse colon with extensive pneumoperitoneum (Fig. 2B).

Chest anteroposterior showing extensive free air (white asterisks) in the subphrenic area.

Computed tomography findings. (A) Wall defects (white dots) were seen at the rectum with abundant fecal material (white asterisks) in the pelvic cavity. (B) Extensive free air on peritoneal cavity (white asterisk) and Subserosal pneumotosis (white dots) on descending colon was seen.
An emergent exploratory laparotomy was performed under general anesthesia in the supine position. On opening the abdomen, a large amount of air gushed out and a large amount of fecal material was found. A longitudinal, 10 cm, full-thickness perforation at the rectum was seen at 5 cm above the peritoneal reflection. Multiple subserosal tears were seen in the sigmoid colon and descending colon, and an approximately 15-cm-sized serosal and muscle layer tear was seen in the splenic flexure of the colon (Fig. 3). Anterior resection with a left hemicolectomy, and temporary colostomy of the transverse colon was decided as the best treatment approach. The postoperative course was uneventful, and he was discharged on the 12th day postoperatively.
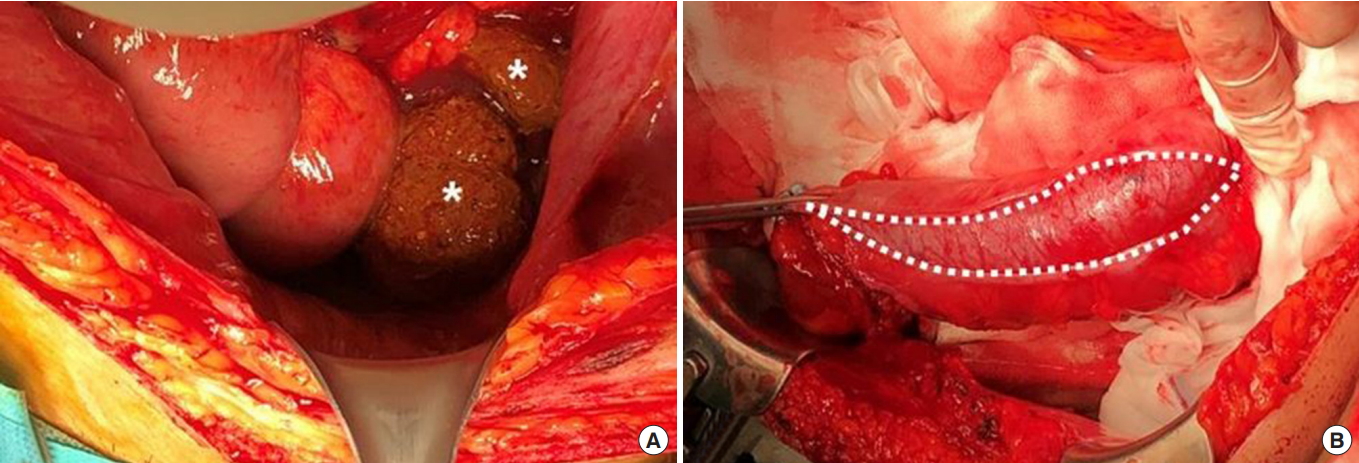
Operative findings. (A) A large amount of fecal material (white asterisks) was found in the pelvic cavity due to rectal perforation. (B) Longitudinal serosal tear of the left colon (white dots).
DISCUSSION
Pneumatic colon injuries have been reported historically, first by Stone in 1904 [3], and similar cases have been reported sporadically. These injuries are generally caused by industrial injury, and primarily occur as a result of practical jokes [4]. As mentioned earlier, pneumatic colorectal injury can occur without inserting the air hose into the anus. High pressure compressed air can form a column, which acts like a solid body, which forces the anal sphincter open [5]. The compressed air concentrated around the anus can easily be delivered through the anus, because of the funnel-shaped anatomical structure of buttocks. Therefore, the compressed air could easily pass through clothes, and even the anal sphincter, and then cause colorectal injury [1].
The normal colon can withstand high intraluminal pressure before rupture occurs. When pressure progressively increases, serosal tear occurs first, followed by the muscle and the mucosa [6, 7]. Colonoscopic studies have found that the intraluminal pressure required to perforate the colon was greater than 0.109 kg/cm2 (1.547 psi/80 mmHg) [8]. In the cadaveric sigmoid colon, a serosal tear can occur with a pressure of 0.27 ± 0.02 kg/cm2 (3.9 ± 0.29 psi/ 202 ± 15 mmHg), and a mucosal rupture can be caused by pressure of 0.307 ± 0.019 kg/cm2 (4.32 ± 0.271 psi/ 226 ± 14 mmHg) following colonoscopic insufflations [9]. In industrial fields, highly compressed air over 10 kg/cm2 , is widely used which is greater than the pressure needed for intestinal perforation [1].
Severe abdominal distension, pain, and peritoneal signs such as abdominal rigidity, tenderness, and rebound tenderness are common clinical manifestations [10]. The diagnosis is usually straightforward because the patient typically has a history of abdominal pain and distension after exposure to compressed air. In addition, a distended colon or a large amount of free air in the peritoneal cavity could be observed by chest or abdominal radiologic examinations [1]. This patient also complained of abdominal distension, pain, peritoneal signs, and a large amount of free air. Although the patient exhibited tachypnea (respiratory rate 28 breaths/min), other vital signs were stable. Tension pneumoperitoneum may cause respiratory distress and hemodynamic instability. Percutaneous decompression with a needle or cannula may be useful for relieving tension pneumoperitoneum [6, 10].
The anal canal and distal rectum are well-supported by external structures including the endopelvic fascia, or pelvic diaphragm. The rectosigmoid region is the first part of the colon that is impacted by a column of air [2]. Therefore, most reported injuries occur in the rectosigmoid junction, sigmoid colon, and sigmoiddescending junction [2, 6, 7]. We performed APCT before surgical exploration to determine the specific colon injury locations. Unlike previous reports, the perforation was seen in the rectum; however, multiple serosal, mucosal tears were seen in the sigmoid to distal transverse colon. Treating colon perforation is dependent on the extent of contamination [10]. Recently, primary repair of all colorectal injuries has been supported by research studies [11, 12]. However, there is still a debate about the options for primary repair or diversion. At the laparotomy for this case, primary repair was not appropriate because of the length of perforation, multiple subserosal tears, and severe fecal contamination. However, for similar cases the prognosis has generally been favorable in recent reports when early surgical management is performed [1, 2, 7].
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.