INTRODUCTION
Pelvic kidney is an ectopic renal mass with a congenitally short ureter and an aberrant blood supply. It results from failure of the embryonic renal tissue to ascend from its pelvic position to the lumbar region (just inferior to the adrenal gland) during the first 6 to 9 weeks of human development [1]. It is a rare condition with an incidence of 1 case per 2,000 population [2]. Here, we report the safe completion of a laparoscopic anterior resection in a patient with an ectopic pelvic kidney. This case report with written informed consent was approved by the Institutional Review Board committee of the Chung-Ang University Hospital (No. 1803-003-16149).
CASE REPORT
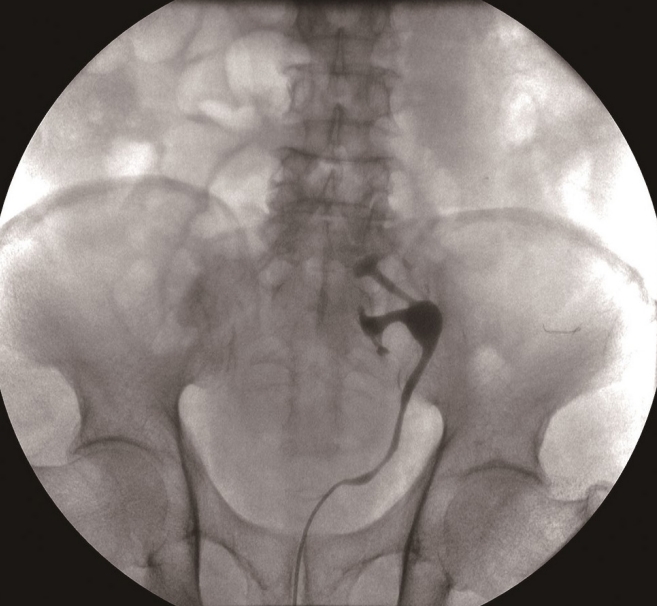
A 76-year-old man visited our hospital with a 2-month history of hematochezia and tenesmus. Otherwise, he took no medications and had no underlying diseases. Colonoscopy revealed an ulcerofungating mass on the distal sigmoid colon. Histopathological examination confirmed a moderately differentiated adenocarcinoma. Computed tomography (CT) of the chest and abdominopelvic area revealed no suspicious metastatic lesion. However, the left kidney was ectopically located in the pelvis, unlike the right kidney (Fig. 1). Specifically, the left kidney was located in the presacral area between the bilateral common iliac arteries, and the direction of its hilum was toward the left common iliac arteries (malrotated). His serum creatinine level was 1.16 mg/dL, and the estimated glomerular filtration rate was 61.21 mL/min/1.73 m2. His serum carcinoembryonic antigen and carbohydrate antigen 19-9 levels were 3.79 ng/mL and 8.50 U/mL, respectively. CT angiography revealed dual main renal arteries from the aortic bifurcation and left common iliac arteries (Fig. 2). A single renal vein drained to the inferior vena cava over the pelvic kidney. The left ureter was relatively short and continued down to the bladder along the lateral pelvic wall (Fig. 3), and a ureteral catheter was placed to identify and preserve the ureter during surgery.
The anterior resection was performed laparoscopically with 4 ports placed as usual (umbilical, right upper, right lower, and left). The left ectopic kidney was identified in the presacral area, and it was covered by the mesentery of the sigmoid colon (Fig. 4A). Dissection was started at the origin of the inferior mesenteric artery (IMA) to prevent injury to the renal arteries. The IMA was ligated at the root of origin (Fig. 4B). Careful dissection to prevent renal vessel damage and to keep the mesocolic fascia intact was continued. After left colon mobilization, the ectopic kidney and its renal vessels were identified within the retroperitoneal tissues without any injury (Fig. 4C). Then, the usual anterior resection was performed. Transection using a linear stapler at the proximal rectum, mini laparotomy at the umbilicus, specimen extraction, and intracorporeal anastomosis using a circular stapler were also performed. After the intravenous injection of indigo carmine, the safety of the ureter was confirmed. In addition, there was no active bleeding around the renal arteries during the operation.
The patient was discharged on postoperative day 8 without any postoperative complication. No deterioration of renal function was observed after surgery. The patient did not receive any adjuvant treatment for low-risk stage IIA colon cancer and was followed up in accordance with the National Comprehensive Cancer Network surveillance guideline [3].
DISCUSSION
The position of the pelvic kidney varies from the iliolumbar area, in the iliac fossa, and over the sacrum to below the pelvic brim [4]. The left-sided kidneys are slightly higher than those on the right. [5]. Blood supply to the pelvic kidney is highly variable, and a more caudally located kidney has the likelihood of multiple vasculatures. In one study, 51.5% of patients had a solitary renal artery arising from the aortic bifurcation, 36.4% had dual arteries arising from the aortic bifurcation and common iliac arteries, and 9.1% had triple arteries arising from the aortic bifurcation, common iliac arteries, and hypogastric artery [4]. Moreover, venous drainage was generally to the common iliac vein and/or distal vena cava. The ureter is usually short, entering the ipsilateral side of the bladder with a normal-appearing intravesical orifice [6]. In contrast to the horseshoe kidney, fusion abnormality is not present in the pelvic kidney.
Laparoscopic colectomy has been a standard treatment for colon cancer, and its advantages include oncological safety, less pain, and early rehabilitation [7]. Sometimes, an unexpected intraoperative event might lead to conversion to open surgery, which diminishes the treatment benefits. Two cases of open conversion during laparoscopic anterior resection because of unexpected ectopic pelvic kidney have been reported [8, 9]. One was performed owing to the possibility of injury to the unidentified vasculature [8]. The author of the study recommended that hand-assisted laparoscopic surgery with laparoscopic ultrasonography could be a feasible procedure. The other conversion was performed to resect the pelvic renal artery, which was confused with the IMA [9]. The author recommended that 3-dimensional CT angiography or magnetic resonance angiography would help to safely perform laparoscopic surgery.
In the present case, CT angiography was performed preoperatively, and it revealed the exact location of the pelvic renal arteries and veins. A conventional abdominopelvic CT scan for the staging workup might not be adequate, because it is not able to determine the explicit number of pelvic renal arteries and their location. Preoperative retrograde pyelography to identify the location of the ureter and ureteral catheter insertion to prevent injury to the ureter were also helpful. Given the preoperative understanding of the positional relationship and the detailed locations, laparoscopic anterior resection in a patient with pelvic kidney could be performed without the risk of injury to the pelvic kidney.
Some studies report the importance of anatomic considerations of the pelvic kidney in patients with other clinical conditions. Hollis et al. [6] reported various surgical techniques for abdominal aortic aneurysmal repair according to the anatomic location of the pelvic kidney. There is a case report of pelvic kidney that was misinterpreted as bulky lymph node conglomerates in 2 patients undergoing gynecological surgery [10]. The authors highlight the need for awareness of the pelvic kidney and its accurate anatomic location. Tsao et al. [11] described a patient with pyelonephritis in a right-sided pelvic kidney who initially presented with the clinical and laboratory features of perforated appendicitis.
Total mesorectal excision is a standard technique for the treatment of rectal cancer [12]. It is a precise dissection of the rectum with intact proper rectal fascia to remove possible metastatic lymph nodes. Complete mesocolic excision for colon cancer is a similar concept to total mesorectal excision in surgery [13]. This procedure also removes the mesocolon with intact proper colic fascia and leaves the intact retroperitoneal fascia over the ureter, hypogastric nerve, and gonadal vessels. In the present case, the vasculature and ectopic kidney were partially visualized within the retroperitoneal fat below the intact retroperitoneal fascia during the operation. The effort of the surgeon to keep the proper colic and retroperitoneal fasciae intact, according to complete mesocolic excision, could lead to the safe completion of a laparoscopic colectomy.
This report presents a case of laparoscopic anterior resection that was safely performed without conversion to open surgery in a patient with a pelvic ectopic kidney. An adequate preoperative evaluation that supplies knowledge about the pelvic kidney and its anatomical relationships is essential to prevent injury to the pelvic kidney. Effort to keep the oncological surgical plane could also lead to completion of laparoscopic surgery.