Delorme's Procedure: An Effective Treatment for a Full-Thickness Rectal Prolapse in Young Patients
Article information
Abstract
Purpose
Delorme's procedure is infrequently applied in young adults because of its assumed higher recurrence rate. The aim of this prospective study was to assess the efficacy of the Delorme's technique in younger adults.
Methods
Fifty-two consecutive patients were entered in our study. We followed patients for at least 30 months. Their complaints and clinical exam results were noted.
Results
Our study included 52 patients (mean age, 38.44 years; standard deviation, 13.7 years). Of the included patients, 41 (78.8%) were younger than 50 years of age, and 11 (21.1%) were older than 50 years of age. No postoperative mortalities or major complications were noted. Minor complications were seen in 5 patients (9.6%) after surgery. The mean hospital stay was 2.5 days. In the younger group (age ≤50 years), fecal incontinence was improved in 92.3% (12 out of 13 with previous incontinence) of the patients, and recurrence was seen in 9.75% (4 patients). In the older group (age >50 years), fecal incontinence was improved in 20% (1 out of 5 with previous incontinence) of the patients, and recurrence was seen in 18.2% (2 patients). In 50% of the patients with a previous recurrence (3 out of 6 patients) following Delorme's procedure as a secondary procedure, recurrence was observed.
Conclusion
Delorme's procedure, especially in younger patients, is a relatively safe and effective treatment and should not be restricted to older frail patients. This procedure may not be suitable for recurrent cases.
INTRODUCTION
A full-thickness rectal prolapse is a formidable and debilitating condition that needs surgical management. It can usually be easily diagnosed with a careful history and physical exam. The associated symptoms are tenesmus, incomplete evacuation, obstructed defecation, mucus discharge, bleeding, the need to manually assist in defecation by pushing in the perineum, and functional complaints like incontinence, constipation and even diarrhea.
More than 100 procedures have been described for the correction of rectal procidentia [1], but no clear procedure of choice exists. The aim of treatment is to repair the prolapse and to resolve functional problems like incontinence and constipation with a low complication rate, an acceptable mortality rate, and a low recurrence rate [2, 3]. Delorme's procedure was initially described in 1900 as a technique to correct an overt rectal mucosal prolapse [4].
Perineal procedures such as the Delorme's technique are reserved for older frail patients with significant comorbidity because a higher recurrence rate is assumed when using perineal procedures [5-7]. However, the recurrence rate in younger (≤50 years of age) patients who undergo Delorme's procedure has recently been shown to be comparable with those of transabdominal approaches [8]. Moreover, neurologic complications (including sexual or urologic disturbances) related to extensive dissection within the pelvic region have been reported in transabdominal approaches. This study was performed to investigate the effectiveness of Delorme's procedure and to review the clinical outcomes for patients who underwent that procedure, with a special focus on patients 50 years of age or younger.
METHODS
Our study was a prospective descriptive study conducted from 2009 to 2012. Fifty-two consecutive patients who had undergone Delorme's procedure for treatment of full-thickness rectal prolapses with diameters of 2 to 12 cm were included in the study. Patients with a history of treatment failure with other procedures, including Delorme's procedure, were also included. Patients who had undergone a modified Delorme's procedure were excluded. Preoperational defecography was done in a group of patients, and proctoscopy, rectosigmoidoscopy or anal manometry were done selectively. A complete history, including symptoms, signs, family history, and past surgeries, was taken before the operation. Patients were considered continent if they could hold air, liquid, and solid.
Preoperative mechanical bowel preparation with a polyethylene glycol solution, preoperative administration of an antibiotic preparation of oral erythromycin or metronidazole, and administration of postoperative intravenous antibiotics (three doses) were used in all of patients. Preoperative anticoagulation therapy was administered for deep venous thrombosis prophylaxis if indicated. All the patients signed an informed consent form before surgery. Patients were positioned in the lithotomy position. Spinal anesthesia was carried out in 40 cases (77%), and general anesthesia was done in 12 (23%) according to patient's will.
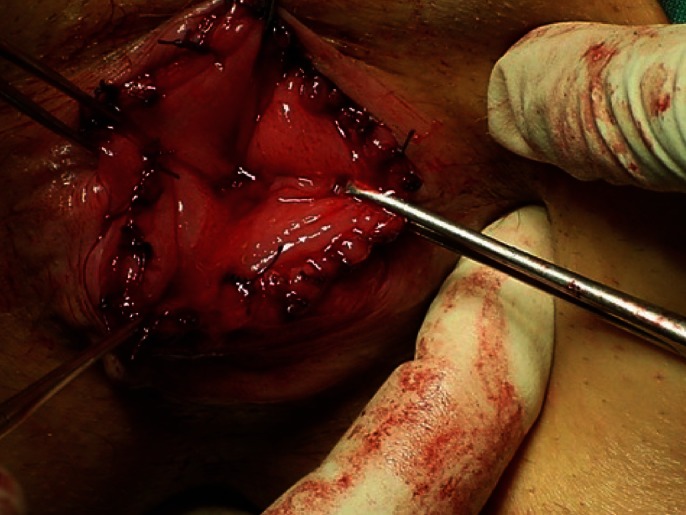
The standard Delorme's procedure was used. The prolapse was fully extended, and a circumferential mucosal incision, about 2 centimeters above the dentate line, was made after injection of epinephrine solution (1:100.000) into the submucosa. The mucosa was dissected from the muscularis layer. The exposed muscular layer was then folded, and eight plicating sutures of long-acting absorbable material were inserted in the muscular wall of the rectum and then gently tied. Eventually, the cut ends of the mucosa were sutured together.
The patients were usually helped out of bed the evening of the surgery and were fed orally within the first 24 hours after surgery. The discharge date was determined based on the patient's medical condition and complications. On discharge, patients were educated about dietary fiber and adequate fluids. All patients were followed up for at least 30 months postoperatively, trimonthly in the first year and then every 6 months. During the follow-up period, data were collected in the presence of a colorectal surgeon. All patients were questioned about improvements of symptoms or any complaints and were examined. A recurrence was defined as a full-thickness protrusion of the rectal wall discovered upon examination.
RESULTS
Our study included 52 patients (31 males and 21 males; male: female ratio, 1.47:1) (Table 1). Two of them had a family history of full-thickness rectal prolapse in their first-degree relatives. The mean hospital stay was 2.5 days. Twenty-one patients (40.3%) had a history of past anorectal surgeries, including surgical repair of a rectal prolapse (n = 6, 4 abdominal procedures and 2 Delorme's procedures), a hemorrhoid (n = 8), a perianal abscess or fistula (n = 3), a pilonidal sinus (n = 2), an anal fissure (n = 1) or a rectovaginal fistula (n = 1). On the preoperative pelvic examination, 23 patients (44%) had a large prolapse (diameter, >5 cm), and 29 (56%) had a small prolapse (diameter, <5 cm).
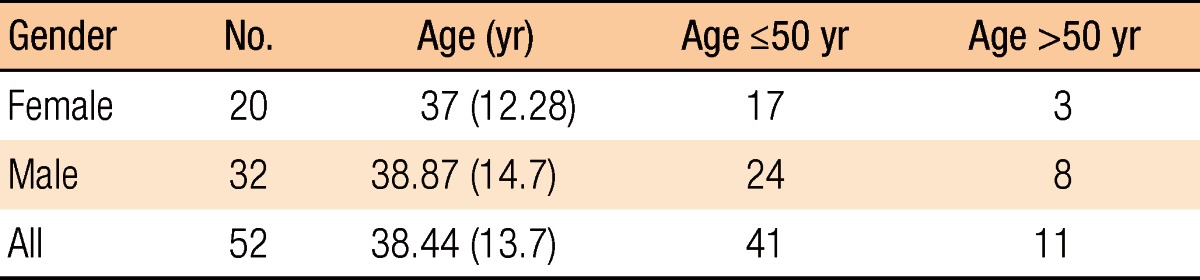
Demographic information on the patients
No perioperative deaths and no intraoperative complications were noted. Minor postoperative complications occurred in 8 patients (15.4%); 4 patients (7.7%) had urinary retention requiring short-term catheterization, and 4 patients (7.7%) had minor surgical site bleeding (one after 7 days). All eight patients with minor postoperative complications were treated conservatively. No dehiscence, hematoma, cellulites or strictures were noted.
The types and prevalences of symptoms at the times of the follow-up visits are summarized in Tables 2 and 3. Eleven of the 52 patients (21%) had complained of exclusive gas incontinence preoperatively, and 7 of the 52 (13.4%) had had solid incontinence and soiling (mucus discharge). Solid incontinence was always associated with gas incontinence. On the first follow-up visit after surgery, 12 of the patients exclusively had gas incontinence (2 new incidences after surgery); however, the prevalence decreased to 7, 4 and 3 persons by the ends of the first, second and last follow-up visits, respectively. No new incidents of gas incontinence were noted at the last follow-up visit. Fecal incontinence was still present in four patients on the first follow-up visit after surgery (three with a history of incontinence before surgery), two of which were found to be continent on the last follow-up visit. Incontinency was resolved in 92% of the patients in the younger group and was improved in 60% of the patients in the older group (Fig. 1). The preoperative constipation and cure rates are shown in Table 3. Two of the 52 patients had had sexual complaints before surgery: a 27-year-old man with a history of impotence and dry ejaculation after an abdominal repair of a rectal prolapse and a 62-year-old man with 2 years of impotence and decreased libido and with a 4-year history of a rectal prolapse.

Preoperative and postoperative incontinence in the patients

Preoperative and postoperative incontinence among two age groups

Incontinence cure rate in two different age groups.
In 3 of the 6 patients (50%) with recurrence, Delorme's procedure as a secondary procedure after the primary procedure (2 abdominal procedures and 1 previous Delorme's procedure) had failed. In the other 3, 1 of whom had had a past history of anal fissure repair, Delorme's procedure was a primary procedure. Four of the 6 patients with recurrence underwent further surgery (1 abdominal procedure, 1 Delorme's procedure, 2 Altemeire procedures); and 2 of the 6 did not desire additional treatment because of the annoyance (Kaplan-Meier curve).
DISCUSSION
Our study prospectively evaluated the anatomical and the functional outcomes (and showed the efficacy) of Delorme's procedure in patients with a full-thickness rectal prolapse. Figs. 2 to 6 depicts the procedure in detail. To our knowledge, only a few studies have been published on the efficacy of Delorme's procedure in the repair of a rectal prolapse in young patients [8, 9]. Surgical techniques used to repair rectal prolapse are generally categorized into perineal or abdominal approaches. Abdominal procedures mainly involve fixation of the rectum to the sacrum with or without resection of the rectum or the sigmoid colon. The method used for rectopexy may vary in different procedures. Constipation is a known complication of abdominal rectopexy; however, a concomitant sigmoid resection may decrease the constipation rate [10, 11]. Bruch et al. [12] also suggested that preservation of the "lateral ligaments" might improve the postoperative constipation. In addition to the general hazards of laparatomies, these procedures involve the risk of pelvic nerve damage, which may cause sexual dysfunction in men, and adhesion formation, which may affect fertility in women. In one study, retrograde ejaculation and impotence were seen in 17.2% of the patients and were major causes of dissatisfaction after posterior rectopexy [3]. Perineal procedures have been suggested as initial options in certain groups of patients: young men in whom pelvic dissection and associated risk of injury to the pelvic nerves may hazard sexual dysfunction [13, 14], young nulliparous women in whom potential injury to the ovaries and the fallopian tubes should be avoided [15, 16], and frail, debilitated patients who are not suitable for a transabdominal approach.

Injection of epinephrine solution (1:100.000) into the submucosa in patients with a full-thickness rectal prolapsed.

Outcome following the surgery.
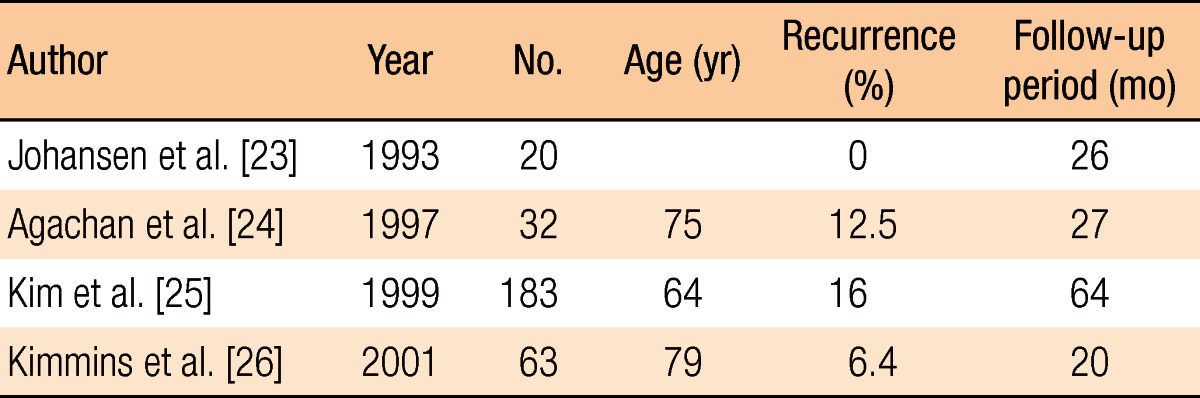
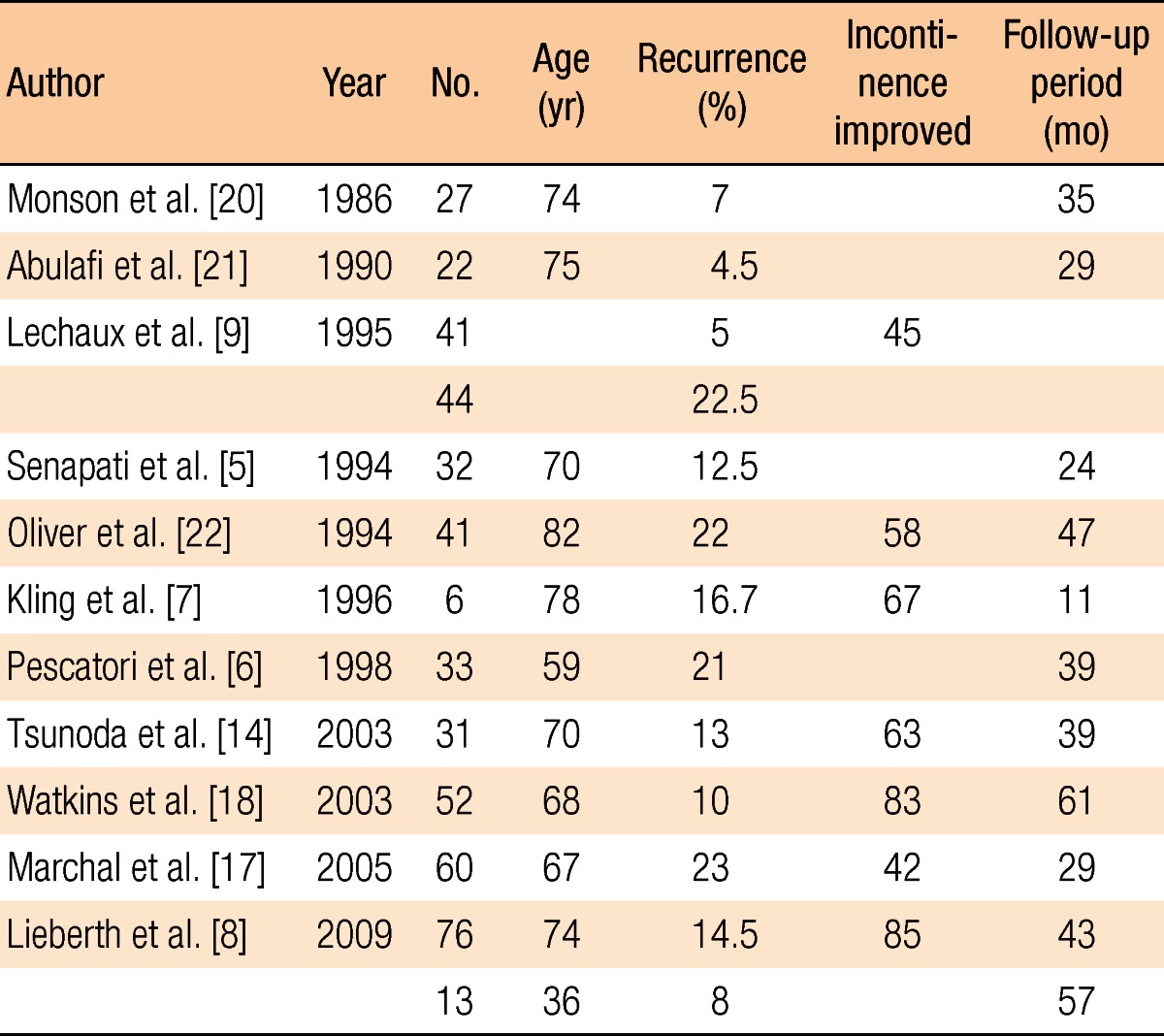
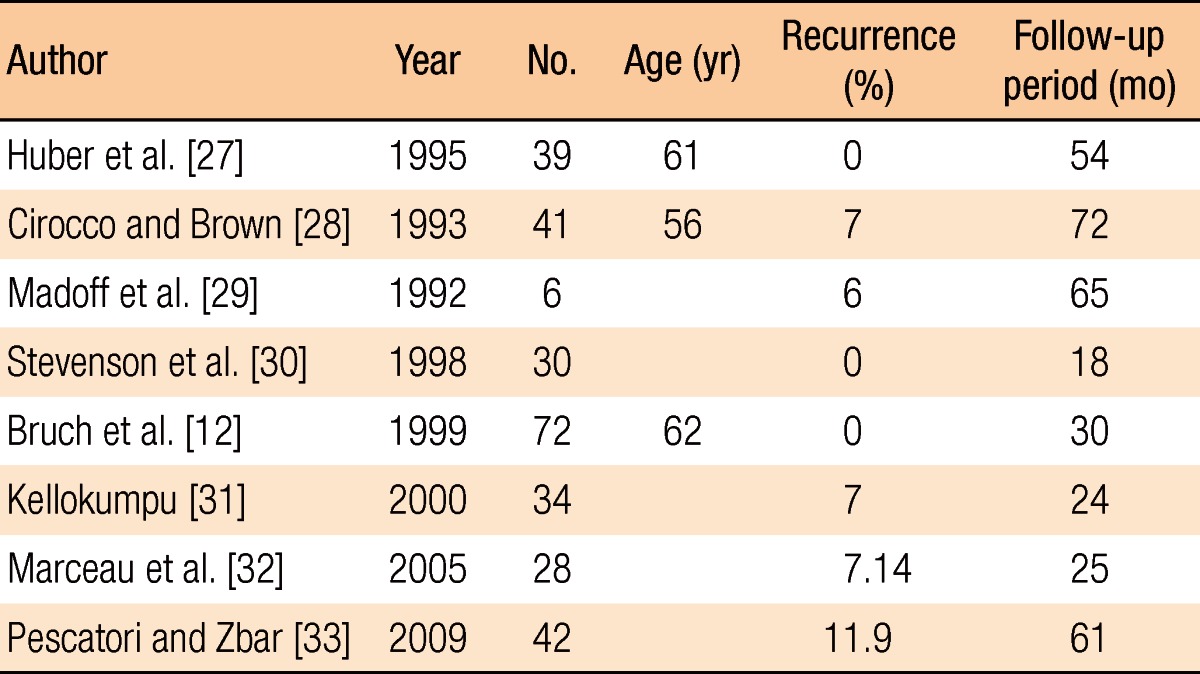
Traditionally, the recurrence rate has been the most important issue in determining the procedure, but recently, functional outcome, operational morbidities and overall costs have been considered. So far, abdominal procedures have been thought to have lower recurrence rates [6, 10, 17]. The various available abdominal procedures have recurrence rates between 0% to 11.9% (Table 3). The recurrence rates in Delorme's procedure and the Altemeire procedure are between 0% to 16% and 4.5% to 23%, respectively (Tables 4-6). The wide variability of reported recurrence rates may be due to different follow-up periods and patient selection. Prior studies reporting high recurrence rates for Delorme's procedure made its less popular and caused it to be reserved for older, medically-unfit patients [18]. Thus, many studies comparing the results of abdominal and perineal procedures suffer from selection bias. If recurrence rates are statistically corrected for age and medical condition, the differences may not be significant.
Delorme's procedures for rectal prolapse
Transabdominal resection procedures
Recent studies on Delorme's procedure have reported low recurrence in young patients [8, 9]. The recurrence rate of 9.75% in our young group is comparable with those of popular transabdominal procedures. With success rates comparable to abdominal procedures, it may be reasonable to use Delorme's procedure as the first choice in the treatment of a full-thickness rectal prolapse in all patients. However, the improvement rates varied dramatically between our groups. The functional outcomes and the complication rate in our young group were more favorable than they were in our older group, with the patients in our older group showing results similar to those in previously published reports. Delorme's procedure is a fast and easy procedure that can be carried out under any type of anesthesia (even local). Lower operative risk, lack of abdominal-surgery complications and quicker recovery make it a safe choice. There is rarely need to wait for ileus resolution, and the time interval before stool passage is often much shorter than it is in abdominal procedures [19]. The shorter hospital stay and the earlier return to work result in a lower cost. With a lower, but acceptable, incontinence improvement, reported to range from 45% to 85%, and a lower postoperative constipation rate, Delorme's procedure has an encouraging functional outcome and is even used for symptomatic relief in constipated patients. Despite the efficacy of Delorme's procedure in treating a primary prolapse, the success results in secondary cases are disappointing. Some investigators have reported high recurrence rates of 47-50% for repeated Delorme's procedures [15, 17]. Surprisingly, even in our young population, the recurrence rate for the secondary procedure was 50%. Consequently, an abdominal repair is suggested for further surgical treatment in recurrent cases, especially in medically-fit patients.
In conclusion, the most appropriate surgical procedure in the treatment of complete rectal prolapse is a matter of controversy. The surgeon should balance the related hazards and advantages in selecting the procedure. Our results indicate the efficacy of Delorme's procedure and its significantly better functional outcome and recurrence rate among young patients. With its minor complications, acceptable recurrence rate and good functional results, we believe that Delorme's procedure should be considered as the first choice for all patients, particularly young adults, presenting with a complete rectal prolapse. Transabdominal techniques may be considered in recurrent cases because of the high recurrence rate for secondary Delorme's procedures.
Notes
No potential conflict of interest relevant to this article was reported.