The Role of Diverting Stoma After an Ultra-low Anterior Resection for Rectal Cancer
Article information
Abstract
Purpose
A diverting stoma is known to reduce the consequences of distal anastomotic failure following colorectal surgery. The aim of this study was to evaluate the efficacy of a diverting stoma after an ultra-low anterior resection (uLAR) for rectal cancer.
Methods
Between 2000 and 2007, 836 patients who underwent an uLAR were divided into two groups, depending on the fecal diversion: 246 received fecal diversion, and 590 had no diversion. Patient- and disease-related variables were compared between the two groups.
Results
Thirty-two of the 836 patients (3.8%) had immediate anastomosis-related complications and required reoperation. Anastomosis leakage comprised 72% of the complications (23/32). The overall immediate complication rate was significantly lower in patients with a diverting stoma (0.8%, 2/246) compared to those without a diverting stoma (5.1%, 30/590; P = 0.005). The fecal diversion group had lower tumor location, lower anastomosis level, and more preoperative chemo-radiation therapy (P < 0.001). In total, 12% of patients in the diverting stoma group had complications either in making or reversing the stoma (30/246).
Conclusion
The diverting stoma decreased the rate of immediate anastomosis-related complications. However, the rate of complications associated with the diverting stoma was non-negligible, so strict criteria should be applied when deciding whether to use a diverting stoma.
INTRODUCTION
Following the introduction of circular staplers in the 1970s and the double stapling technique in the 1980s, the low colorectal anastomosis became a common procedure and is now regarded as routine. A stapled anastomosis is safe, effective, and easy to perform. A major advantage of this technique is that it is performed under direct vision without the impediment of pelvic tissue [1-3]. For a routine low anterior resection, a diverting stoma is not typically necessary. However, the risk of complications, such as leakage, a major adverse event [4], stricture, and fecal incontinence, increases in cases involving sphincter-saving surgery for mid to lower rectal cancer due to the lower level of the anastomosis. Furthermore, anastomotic leakage after rectal cancer surgery has been associated with poor survival [5, 6].
Risk factors contributing to anastomosis leakage include male gender, malnutrition, preoperative weight loss, cardiovascular disease, steroid use, perioperative blood transfusion, advanced age, obesity, previous irradiation, and a low level of anastomosis [5, 7-12]. It has been argued that a diverting stoma is an effective and safe procedure to prevent anastomosis leakage after sphincter-saving surgery [4, 7, 13-17]. However, it has been reported that a diverting stoma may not prevent postoperative anastomotic leakage [18-20]. Furthermore, systematic reviews have reported that complications related to the closure of a diverting stoma were not negligible [21, 22]. Chow et al. [21] reviewed 48 studies evaluating the complications associated with the reversal of a diverting ileostomy and reported a morbidity rate of 17.3% with a mortality rate of 0.4%. Stoma-related complications included small bowel obstruction (7.2%), wound sepsis (5%), the need for relaparotomy (2.5%), incisional hernia of the stoma site (1.8%), leakage (0-8.3%), prolonged ileus (0.8-13.8%), fistula (0-8.6%), bleeding (0-4%), and intra-abdominal abscess (0-1.4%).
An ultra-low anterior resection (uLAR) is associated with a very low anastomosis level and frequently with preoperative chemoradiation therapy (CRT). These factors often require a diverting stoma to be performed. Therefore, the aims of our study were to assess the complications and the effectiveness of a diverting stoma following an uLAR for rectal cancer.The present study was approved by the Institutional Review Board for Human Research at the University of Ulsan.
METHODS
Eligibility and enrollment
Between January 2000 and December 2007, a total of 836 patients underwent an elective and curative uLAR for rectal cancer at Asan Medical Center. The term 'uLAR' is applied if the rectal dissection proceeds below the pelvic floor or the rectum is excised completely. The median follow-up period was 54 months, with a range of 6-146 months. The patients were divided into two groups: 246 underwent an uLAR with fecal diversion and 590 underwent an uLAR without fecal diversion (see below for selection criteria). Diverting stoma-related complications were divided into two categories: stoma creation and stoma reversal. Demographic, preoperative, operative, pathologic, and follow-up data were available from the medical records and a prospectively managed database.
Surgery
For patients receiving preoperative CRT, which was performed with a total of 40-50.4 Gy with FL (5-fluorouracil + leucovorin) or capecitabin, surgery was performed 5 to 6 weeks after completion of treatment. Eight patients were observed to have symptomatic obstruction during the work-up period and underwent diverting stoma surgery before receiving preoperative CRT and undergoing an uLAR. All operations were performed by colorectal surgeons who had each performed more than 150 mesorectal excisions per year for the previous 5 years. The standard procedure was a total mesorectal excision with autonomic nerve preservation. All patients were anastomosed with a double stapling technique, except for two patients who underwent single stapling and five patients who were hand-sewn. Temporary diverting stomas were created as loop ileostomies in patients with more than one of the following: a very low anastomotic level under considerable tension, poor blood supply, positive air leak test result, preoperative CRT, or severe comorbidity. An ileostomy take down was performed via a functional end-to-end anastomosis by using either a linear stapler or a hand-sewn technique.
Follow-up
Colon studies using water-soluble contrast media and digital rectal examination were performed 3 to 4 months after the uLAR with diverting stoma or approximately 1 month after completion of adjuvant therapy. If the test results were normal and the patient had no evidence of recurrence, closure of the diverting stoma was performed. Conversely, if a leak or stenosis was observed, closure was postponed until the leak had healed or the stenosis had been resolved with one or more dilations.
Anastomotic leakage was defined as peritonitis caused by leakage, pelvic abscess, or discharge of feces from the pelvic drain at any postoperative stage. Immediate anastomosis-related complications included leakage, pelvic sepsis, fistula, anastomosis bleeding, or bowel ischemia within a month from the uLAR.
Stoma-related complications were collected from the medical records and a prospectively managed database. Ileus was considered as either prolonged postoperative ileus or delayed ileus. Prolonged postoperative ileus was specified as a delay of 7 days in passing gas. A prolapsed stoma was defined as the need to manually or surgically reduce the bowel. Patients who had radiologic herniation and complained of discomfort at the stoma site were considered to have an incisional hernia of the stoma repair site.
Statistical analysis
Categorised variables were analysed with the chi-squared (χ2) test. Continuous variables were analysed with the Student's t-test. All numbers are expressed as means ± standard deviations. A P-value of < 0.05 was considered statistically significant. All statistical calculations were performed with IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA).
RESULTS
Differences in patient characteristics in the stoma diversion group
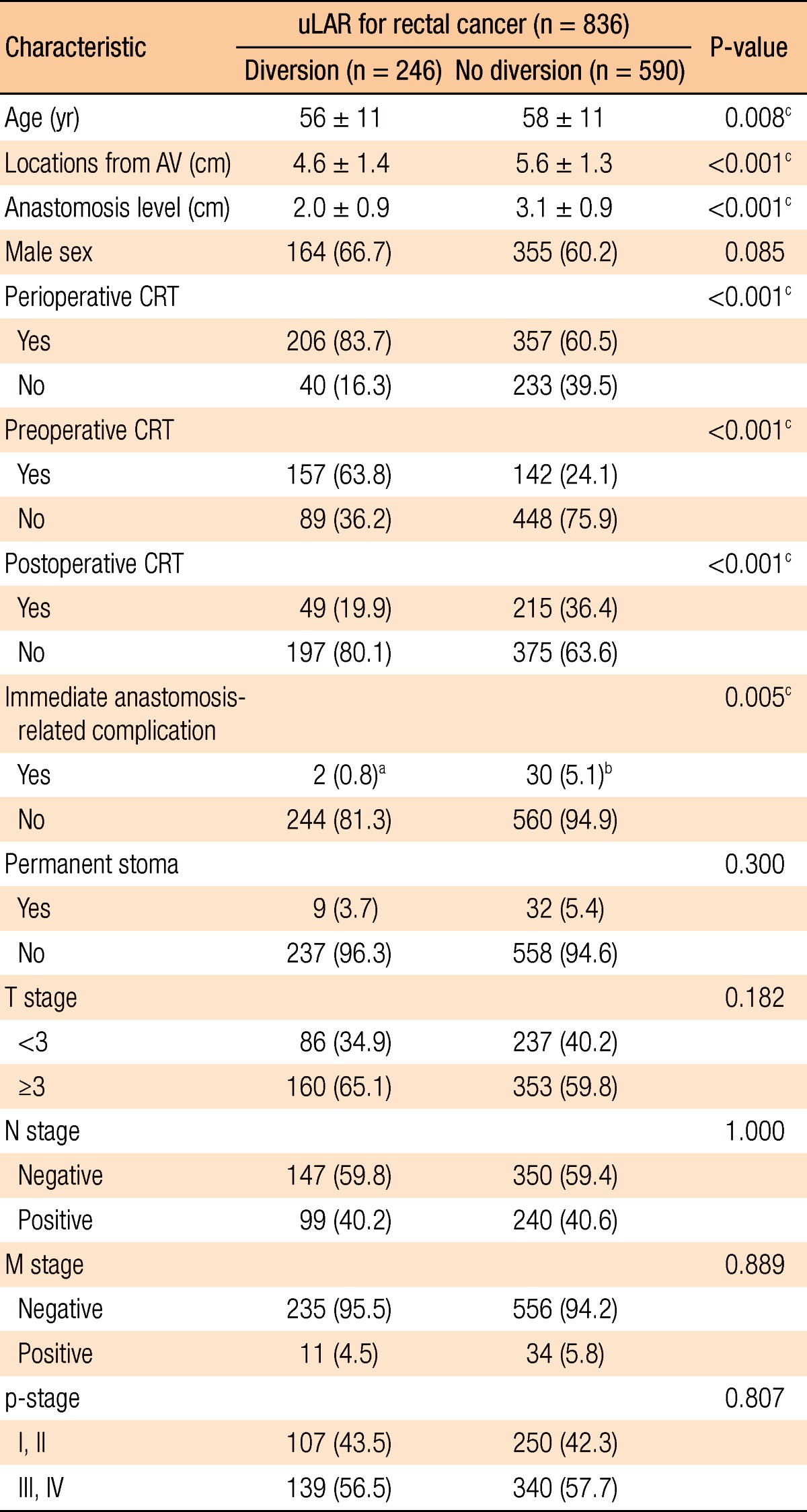
The proportion of men, rate of permanent stoma formation, and pathologic status did not differ between the two groups. However, patients undergoing a diverting stoma were associated with a lower anastomosis level, lower tumor location, higher perioperative and preoperative CRT rates, and lower postoperative CRT rates (P < 0.001). In addition, the median age and rate of immediate anastomosis-related complications were significantly lower for diverting-stoma patients (P < 0.008 and P < 0.005, respectively) (Table 1). The fraction of patients who received preoperative CRT was 36% (299/836). Further, the mean age of the preoperative CRT group was younger than that of the nonpreoperative CRT group (55 years and 58 years, P < 0.001). Approximately half (53%, 157/299) of the patients who received preoperative CRT underwent a diverting stoma. Patients with diversion had lower pelvic sepsis rates than those without it, but the difference was not significant (1.3% vs. 4.9%, P = 0.091).
Patient demographics and perioperative details
Diversion timing and permanent stoma
A total of 275 patients received a diverting ileostomy, followed by a second procedure for stoma closure. Prechronous or synchronous diversion was performed in 246 patients. Only one patient did not undergo a diverting-stoma reversal. A further 30 patients that initially did not receive a diverting stoma underwent the procedure following anastomosis-related complications, and 29 out of the 30 patients (97%) received a stoma reversal (Fig. 1). The durations to diverting stoma reversal were similar, irrespective of whether the patient received the diverting stoma as part of the initial anastomosis or due to anastomosis-related complications (7 ± 3 months vs. 7 ± 8 months, P = 0.573).
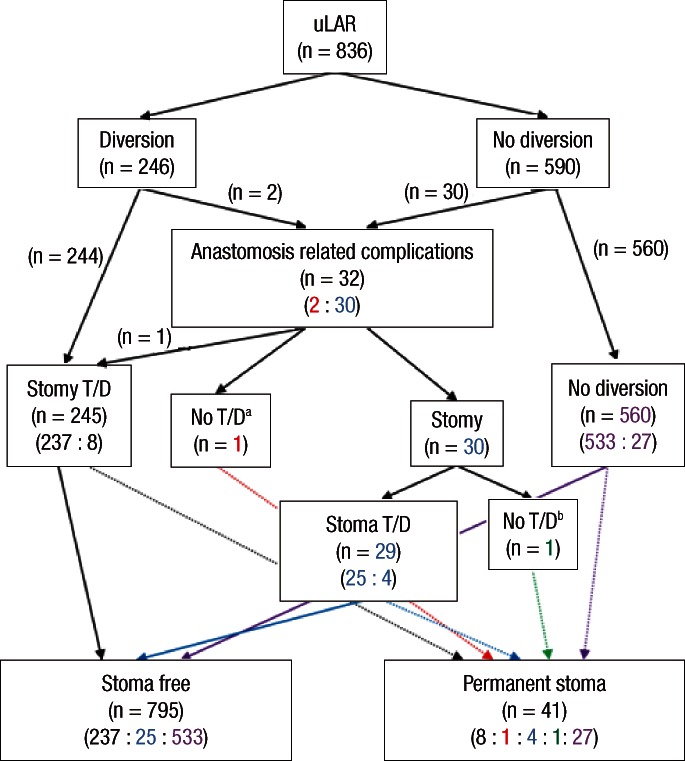
Evolutional changes in stoma status. uLAR, ultra-low anterior resection. T/D, take down. aStoma reversal could not be done because of tumor recurrence. bAnastomosis leakage was continued.
Immediate anastomosis-related complications
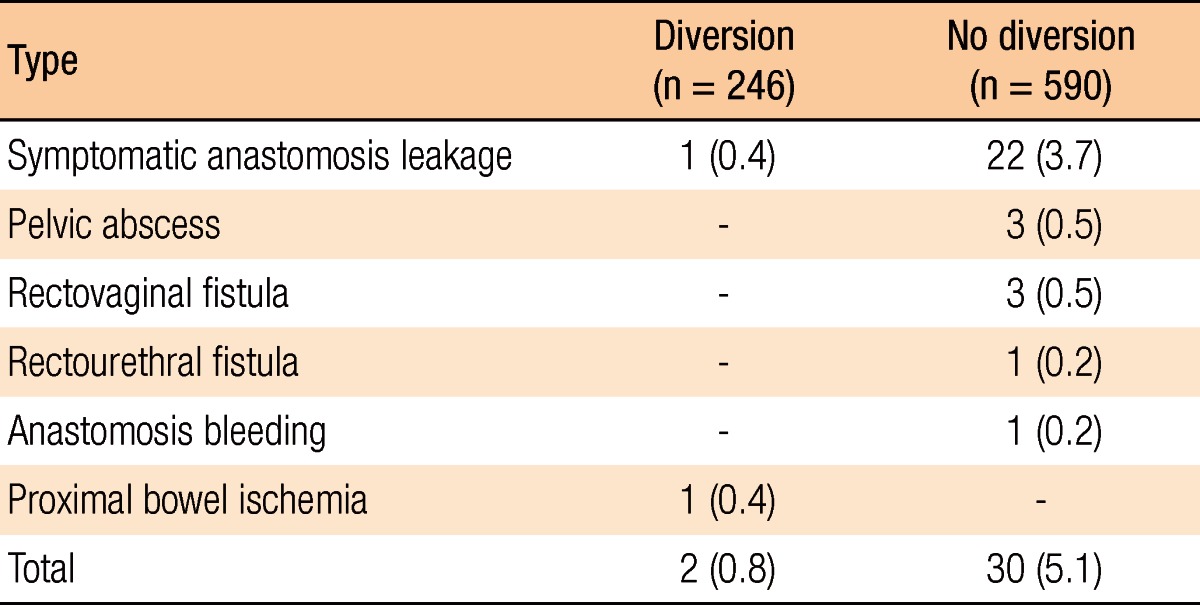
Only 3% of the patients (23/836) suffered symptomatic anastomotic leakage, and 0.8% of the patients (2/246) with a diverting stoma experienced immediate anastomosis-related complications. However, 5.1% of the patients (30/590) without a diverting stoma suffered immediate anastomosis-related complications. Anastomosis leakage comprised 73% (22/30) of the complications. Patients with a diverting stoma suffered lower symptomatic anastomosis leakage rates than those without a diverting stoma (0.4% vs. 3.7%, P = 0.005) (Table 2).
Types of immediate anastomosis-related complications
Diverting stoma-related complications
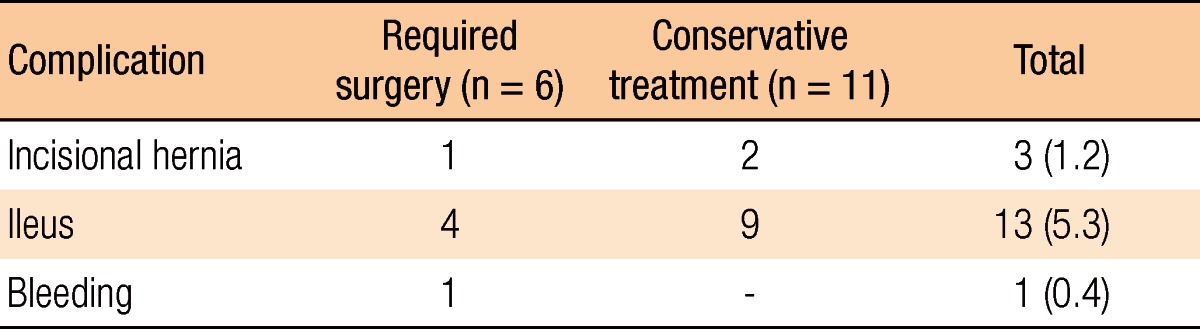
The overall rate of complications following either the creation or the closure of a diverting stoma was 12% (30/246). The overall rate of complications associated with a diverting stoma that required surgery was 5.3% (13/246). After undergoing a diverting stoma, 13 out of 246 patients (5.3%) suffered stoma-related complications. Out of these, a third of the patients required surgical correction (Table 3). The complication rate associated with reversal of the diverting stoma was 6.9% (17/245). The complication rate requiring surgery was also about one third (6/17). The main reason for surgical correction was postoperative ileus (Table 4). There were no mortalities.

Complications associated with creating the ileostomy (n = 246)
Complications associated with reversal of the diverting stoma (n = 245)
DISCUSSION
The total mesorectal excision (TME) technique and preoperative CRT were standard treatments for mid to low rectal cancer. However, they have been associated with an increased risk of symptomatic anastomotic leakage [4, 23]. Symptomatic anastomotic leakage can be a catastrophic complication after sphincter-saving surgery for rectal cancer, with an incidence that has been reported as ranging from 1% to 24% [5, 7, 15, 16, 19, 24, 25]. Mortality associated with anastomotic leakage has been reported as ranging from 2.1% to 22% [7, 16, 19].Furthermore, anastomosis leakage has been reported to be an independent prognostic factor for local recurrence [26, 27]. Jung et al. [5] reported that anastomosis leakage had significantly poorer long-term survival because the adjuvant chemotherapy was delayed or abandoned. Long-term functional outcome is also impaired by anastomotic leakage that reduces neorectal reservoir functions, owing to failure of healing by first intention with granulation tissue formation and consequent fibrosis [28, 29]. In our study, only 3% of the patients (23/836) suffered symptomatic anastomotic leakage, and there were no mortalities. Our leakage rate was very low compared to other studies. Only one of the 246 patients who underwent an uLAR with a diverting stoma could not undergo diverting stoma reversal because of tumor recurrence. These results may be attributed to robust selection criteria that considered high-risk patients and the appropriate use of diverting stoma.
We found that the diverting stoma group had a lower anastomosis level and a higher rate of preoperative CRT. These results may be attributed to our selection criteria. We performed a diverting stoma in cases with more than one of these conditions: a very low anastomotic level under considerable tension, poor blood supply, positive air leak test result, preoperative CRT, and severe comorbidity. Further, the mean age of the diversion group was younger than that of the nondiversion group. This may be due to the more frequent use of preoperative CRT in young patients. Furthermore, the diverting stoma group suffered fewer immediate anastomosis-related complications. We hypothesise that a diverting stoma may be a highly effective modality to prevent clinical anastomotic leakage after an uLAR for rectal cancer, although the younger age of the patients with a diverting stoma may be a factor in its comparative success.
A recent study showed that 19% of patients obtained a permanent stoma after a low anterior resection for rectal cancer, and 56% of the patients with a permanent stoma had previous symptomatic anastomotic leakage [30]. In this study, the rate of permanent stomas was 5% (41/836), and only 15% of the patients (6/41) with a permanent stoma suffered previous symptomatic anastomotic leakage. The main cause of a permanent stoma was recurrence. Only one of 246 patients with a diverting stoma suffered symptomatic anastomotic leakage. However, 3.7% of the patients (22/590) who underwent an uLAR without a diverting stoma had symptomatic anastomosis leakage (P = 0.005).
Our results are in agreement with previous studies on a diverting stoma and its relation to a reduction in anastomosis-related leakage. However, it must be recognized that a diverting stoma requires the patient to undergo two surgeries. Furthermore, some studies have reported considerable stoma-related complication rates [21, 22, 31]. In a recent review of 48 studies, including 6,107 cases, the reported overall morbidity following closure of a diverting stoma was found to be 17.3%, with a mortality rate of 0.4%. The two major postoperative complications were small bowel obstruction and wound sepsis [21]. Our overall rate for stoma-related complications was 12% (30/246), and 5.3% of the patients (13/246) required surgery. There were no mortalities. We found that the rate of stoma-related complications was non-negligible and that the rate of complications for stoma creation and closure was quite similar to those in other studies. The most common complication after stoma reversal was ileus at 5.3% (13/245). In one systemic review, 7.2% of the patients (339/4,735) suffered from small bowel obstruction following ileostomy closure, and a third of those patients (107/339) required a relaparotomy [21]. Our study showed similar data as 31% of the patients (4/9) with ileus after reversal of the diverting stoma required reoperation. Furthermore, three cases of incisional hernia and one case of anastomotic bleeding were identified following stoma reversal. Therefore, reversal of a loop ileostomy requires careful attention to detail to prevent postoperative ileus. We recommend lysis of all adhesions under direct vision and careful reanastomosis, taking care to prevent anastomosis stricture and bleeding.
Complication rates following loop ileostomy construction have been reported as ranging from 4% to 45%, and reoperation rates have been reported to be between 1% and 6% [32-35]. Excluding ileus that was resolved within 3 days and minor wound problems, we found that, similar to other studies, 5.3% of the patients with a diverting stoma (13/246) suffered complications, and the reoperation rate was 2.8% (7/246). This retrospectively designed study has a limitation, possible selection bias, because some patients underwent a diverting stoma based on the final decision of the surgeon, even though some specific conditions for diversion had been recommended.
In conclusion, a diverting stoma could decrease the rate of immediate anastomosis-related complications following an uLAR for rectal cancer. However, the overall complication rates associated with diverting stoma were non-negligible. Judicious patient selection and a meticulous surgical technique are recommended when either creating or closing a diverting stoma following an uLAR.
Notes
No potential conflict of interest relevant to this article was reported.