Treatment Outcomes of Anorectal Melanoma
Article information
Abstract
Purpose
An anorectal melanoma (AM) is a very rare tumor. However, sufficient data supporting effective surgical options for the disease do not exist. This retrospective review aimed to analyze treatment outcomes for an AM.
Methods
From June 1999 to December 2008, we retrospectively reviewed a prospectively collected consecutive series of 19 patients who had undergone a surgical resection for an AM at a single institute. Surgical method and clinicopathological factors were analyzed.
Results
The median age was 61.4 years (range, 46 to79 years). Main symptoms were an anal mass, hematochezia, perianal pain, tenesmus, fecal incontinence, and bowel habit change. The average duration of symptoms before diagnosis was 7.8 months (range, 1 to 36 months). S-100 and HMB-45 were positive in all patients, even in non-melanin pigmentation. There were 12 abdominoperineal resections (APRs) and 7 wide local excisions (WEs). The APR showed longer overall survival when compared with the WE (64.1 months vs. 10.9 months, P < 0.001). No patients who underwent a WE survived more than 13 months.
Conclusion
A high index of suspicion is necessary to establish the diagnosis for an AM in patients with anal symptoms, and S-100 and HMB-45 can be useful markers for an AM. Even with the small number of cases and the short follow-up, our data suggest that an APR for an AM may provide longer survival than a WE.
INTRODUCTION
An anorectal melanoma (AM) has been reported to be a very rare tumor. AM represent only approximately 0.4-0.6% of all melanoma cases [1-3] and 1% of anorectal malignant tumors [4, 5]. Nevertheless, its prognosis is very poor [5, 6].
Since AM do not respond well to chemotherapy or radiation therapy, selection of surgical treatment is considered to be important, and the abdominoperineal resection and the wide excision are possible surgical methods [1, 7, 8]. Traditionally, the abdominoperineal resection has been preferred. Nonetheless, recently, cases treated with only a wide excision have shown outcomes comparable to those achieved when using an abdominoperineal resection [7, 9, 10]. However, studies based on objective data that allow the surgical method to be selected are not sufficient. In our study, the clinical characteristics of an AM were examined, and variations in the treatment outcomes after surgical resection according to the surgery method used were analyzed.
METHODS
Among a total of 2,753 patients diagnosed as having anorectal malignant tumors from June 1999 to December 2008, 19 patients who were definitely diagnosed histologically as having an AM were selected as the subjects of this study (minimal follow-up period, 7 months). In this retrospective study, the medical records of patients were examined, and the characteristic of patients, surgical methods, prognoses, and pathological records were analyzed. For the comparisons of the clinical characteristics of the two groups and of the survival rate, the chi-square test and the Kaplan-Meier test were used.
RESULTS
Among the total 19 patients, 8 patients were males, and 11 patients were females, and their average age was 61.4 years (range, 46 to 79 years). At the time of the visit to our outpatient clinic, common symptoms were rectal tumors (47%), hematochezia (42%), and pain in the anal area (16%). In addition, tenesmus, fecal incontinence, change in bowel habit, etc. were shown. The interval from the onset of symptoms to the diagnosis of an AM was an average of 7.8 months (range, 1 to 36 months).
Among the 19 patients, abdominoperineal resection was performed on 12 patients, and wide excision was performed on 7 patients. Among the 12 patients who underwent an abdominoperineal resection, 4 patients were males, and 8 patients were females. Among the 7 patients who underwent a wide excision, 4 patients were males, and 3 patients were females. The mean ages of the two groups were 59 years and 63 years, respectively. The interval from the onset of symptoms to the diagnosis an AM in the abdominoperineal group was an average of 6.9 months (range, 1 to 24 months), and that in the wide excision group was an average of 8.3 months (range, 1 to 36 months). The average tumor size for the abdominoperineal group was 3.9 cm (range, 0.6 to 4.7 cm), which was bigger than the 2.6 cm (range, 1.2 to 4.5 cm) for the wide excision group, but the difference between the two groups was not statistically significant. The average distance from the anal skin to the tumor for the abdominoperineal resection group was 2.2 cm, and that for the wide excision group was 1.6 cm. Melanization was detected in 12 patients (63%) of the total 19 patients (6 patients in the abdominoperineal resection group, and 6 patients in the wide excision group) (Fig. 1).

Gross finding of anorectal malignant melanoma.
In the abdominoperineal resection group, 33% of the patients (4/12 patients) received postsurgical adjuvant chemotherapy while in the wide excision group in 29% of the patients (2/7 patients) did, and these percentages are not high. Similarly, the percentages of patients receiving postsurgical adjuvant radiation therapy in the two groups were 17% (2/12 patients) and 29% (2/7 patients), respectively; thus, postsurgical adjuvant radiation therapy was not performed aggressively (Table 1).
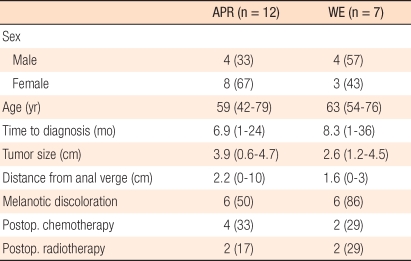
Clinical characteristics of two groups (APR and WE)
For a pathologically definite diagnosis of melanoma, immunohistochemical staining methods were applied. Among the 19 patients, S-100 and HMB-45 staining were performed on 10 patients (Fig. 2). Among the 10 patients, 5 patients showed melanization, and the remaining 5 patients did not show melanization. The results showed that all patients were positive, and even in patients without melanization, positive reactions were detected in immunohistochemical staining.
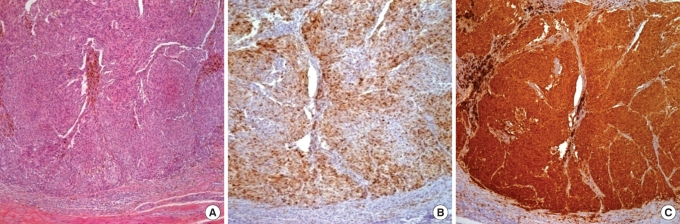
(A) Pathologic finding of anorectal malignant melanoma (H&E, × 100). (B) Pathologic finding of anorectal malignant melanoma (HMB-45, × 100). (C) Pathologic finding of anorectal malignant melanoma (S-100, × 100).
In the comparison of the survival period after surgery, the mean survival period of the abdominoperineal resection group was 66.1 months (range, 9 to 103 months) while that of the wide excision group was 11.2 months (range, 7 to 13 months). The survival period of the abdominoperineal resection group was shown to be significantly longer (P = 0.001) (Table 2).
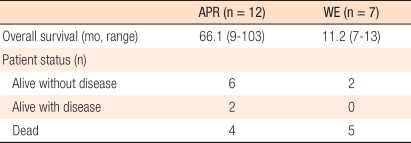
Comparison of survival between two groups (APR and WE)
In the abdominoperineal group, 50% of the patients survived for longer than 5 years. On the other hand, in the group that only underwent a wide excision, including 1 patient who underwent palliative surgery because of multicentric lung and liver metastases, none of the patients survived for longer than 13 months (Fig. 3).

Survival curves of two groups (APR and WE) (P = 0.001).
APR, abdominoperineal resection; WE, wide local excision.
DISCUSSION
An AM is a rare disease [1-3]. In Korea, only a few cases and small scale studies have been reported [11-13]. At our institution, patients who underwent surgery for anal and rectal cancer from 1999 to 2008 totaled 2,753 cases. Among them, only 19 patients were definitely diagnosed pathohistologically as having a melanoma. Because of the small number of patients, it was difficult to validate the statistical significance of the classification of the presurgical clinical characteristics of patients or to compare outcomes according to surgical methods.
In other studies, similarly [1, 14, 15], symptoms that patients presented with most frequently were tumors in the anal area, hematochezia, and pain in the anal area; hence, the patients were misdiagnosed as having a hemorrhoid. Thus, their conditions were not taken to be serious, and treatments were postponed. In addition, at small hospitals, only partial resections were performed in many cases [14]. Therefore, the interval to the initial diagnosis was long, and the AM was not diagnosed appropriately in many cases. This is associated with the poor prognosis of AM [11]. Therefore, when tumors in the anal area are resected, pathohistological examinations should be performed, and based on the results, appropriate additional treatments should be administered if required.
It has been reported that to determine properly the type of surgery for an AM, the age of the patient, the symptoms, and the general conditions, such as the past history, the size and location of the tumor, and the presence or absence of distant metastasis, should be considered [16]; nonetheless, an objective guideline that could help select the surgical method has not been established yet. In our study, similarly, even though a tendency existed to perform a wide excision for cases in which tumors were located close to the anus, cases with small-sized tumors, and cases with relatively mild symptoms, the preferences of patients themselves and/or surgeons were added; thus, an objective indication for surgery could not be shown. Treatment guidelines for patients diagnosed as having an AM must be established through continuous studies in the future and through collaboration with other institutions.
Melanization, which has been considered to be specific for the diagnosis of melanoma in the past [7, 15], was detected in only 63% of the cases (12/19 patients). In macroscopic or endoscopic examination, it should be understood that even cases without melanization could be diagnosed as having a melanoma [7, 15]. In this study, in the pathological diagnosis process, immunohistochemical staining using HMB-45 and S-100 was performed on 10 patients, and regardless of melanization, all cases were found to be positive [17]. HMB-45 melanoma-related antigen is a marker specific to the diagnosis of a melanoma. S-100 protein is a differentiation marker of melanocytes, and its sensitivity has been reported to be high. In addition, mela-A, tyrosinase, and other markers have been used [18]. In the future, use of the immunohistochemical staining technique is recommended for the diagnosis of a melanoma.
In our study, when the survival periods of the patient groups according to surgical methods were compared, all patients surviving for longer than 5 years were patients in the abdominoperneal resection group, and this result was statistically significant. Thus, except for patients whose condition is too poor to perform aggressive surgery, an abdominoperineal resection is advantageous for long-term survival.
To accurately diagnose of an AM and to avoid misdiagnose of patients with anal tumors, hematochezia, pain in the anal area and other symptoms as hemorrhoids or other benign diseases in the anal area, pathohistological tests should be performed. Immunohistochemical staining using markers useful for the diagnosis of melanoma HMB-45 and S-100 is recommended. Although this study was conducted on a small number of patients and the follow up was short, as a surgical treatment for an AM, the abdominoperineal resection showed a longer survival than the wide excision.
Notes
No potential conflict of interest relevant to this article was reported.