Clinical validation of implementing Enhanced Recovery After Surgery protocol in elderly colorectal cancer patients
Article information

Abstract
Purpose
The aim of this study was to evaluate the safety and feasibility of applying enhanced recovery after surgery (ERAS) protocol in elderly colorectal cancer patients.
Methods
The medical records of patients who underwent elective colorectal cancer surgery at our institution, from January 2017 to December 2017, were reviewed. Patients were divided into 2 groups: the young group (YG, patients aged 70 and under 70 years) and the old group (OG, patients over 70 years old). Perioperative outcomes and length of hospital stay were compared between both groups.
Results
In total, 335 patients were enrolled; 237 were YG and 98 were OG. Despite the poorer baseline characteristics of OG, the perioperative outcomes were similar. Length of hospital stay was not different between the groups (YG, 5 days vs. OG, 5 days; P=0.320). When comparing the postoperative complications using the comprehensive complication index (CCI), there was no significant difference (YG, 8.0±13.2 vs. OG, 11.7±23.0; P=0.130). In regression analysis, old age (>70 years) was not a risk factor for high CCI in all patients. In multivariate analysis, C-reactive protein (CRP) level on postoperative day (POD) 3 to 4 was the only strong predictive factor for high CCI in elderly patients.
Conclusion
Implementing the ERAS protocol in patients aged >70 years is safe and feasible. High CRP (≥6.47 mg/dL) on POD 3 to 4 can be used as a safety index to postpone discharge in elderly patients.
INTRODUCTION
Enhanced Recovery After Surgery (ERAS) is a multimodal perioperative care protocol designed for quick postoperative recovery [1, 2]. This protocol reduces surgical stress postoperatively and quickly normalizes the patient’s physiological function. As a result, the recovery period is shortened due to improvement in the immunonutritional status, rapid recovery of bowel function, and reduction of pain. According to several previously published randomized controlled trials and meta-analyses reports, ERAS is known to reduce surgical complications and duration of hospital stay [3-6]. Currently, the ERAS protocol is widely adopted, including at our institution, as a standard treatment option for colorectal cancer patients [5, 7].
Most colorectal cancers occur in the elderly population [8, 9]. Elderly patients need more attention due to a number of factors, including a high prevalence of comorbidities, physiological vulnerability, mental disorders, and poor physical function such as sarcopenia [10]. In order to manage these various problems, a multidisciplinary team approach has advantages. However, there is a lack of studies on the outcomes of implementing ERAS protocols in the elderly population. The aim of this study was to evaluate the safety and feasibility of applying ERAS protocol in elderly colorectal cancer patients.
METHODS
The medical records of patients who underwent elective colorectal cancer surgery at our institution, from January 2017 to December 2017, were reviewed. All patients implemented the ERAS protocol. A group of 23 interventions was applied in this study based on our previously published protocols (Table 1) [7]. Patients who underwent emergency surgery, stoma closure, or transanal local excision were excluded. Tumor location was defined as the right colon (including the cecum, ascending colon, hepatic flexure, and transverse colon) and left colon (including the splenic flexure, descending colon, and sigmoid colon). Tumors located below the peritoneal reflection were defined as rectal. Cancer obstruction was defined as cancer located in the colon and rectum, unable to pass through the lesion by colonoscopy, or exhibiting obstructive findings on computed tomography.
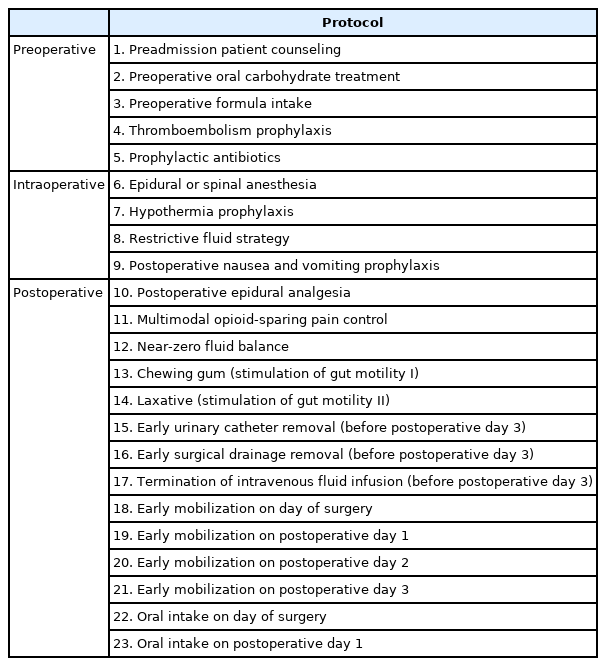
Enhanced Recovery After Surgery protocol for elective colorectal cancer patients
Patients were divided into 2 groups: the young group (YG, patients aged 70 and under 70 years) and the old group (OG, patients over 70 years old). In both of the groups, 237 and 98 patients were registered, respectively (Table 2). Patients’ baseline characteristics, perioperative outcomes, length of hospital stay, and readmission rate were collected. We defined readmission as unplanned readmission within 30 days after discharge.
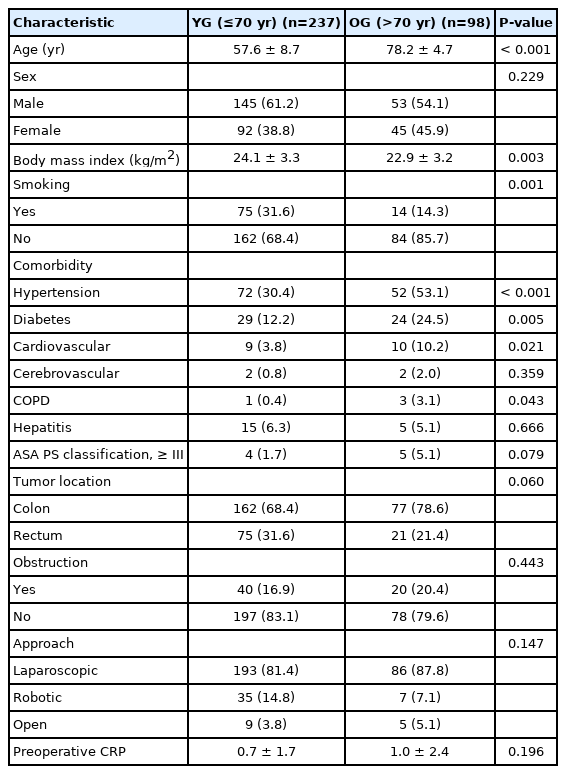
Baseline characteristics of the patients
Complications were evaluated using the comprehensive complication index (CCI). CCI is an alternative tool for evaluating complications. CCI was calculated as the sum of the weighted scores according to the Clavien-Dindo classification (CDC) grade and expressed as a score between 0 and 100. Unlike CDC, CCI can also evaluate all minor complications [11, 12]. CDC grade IIIa or higher is a severe complication that requires intervention, and we used the CCI score of 26.2, which corresponds to 1 CDC grade IIIa, as the cutoff for high CCI based on prior study [13, 14]. All complications that occurred within 30 days after surgery were recorded. The predictive factors associated with the high CCI (≥ 26.2) group were also analyzed.
This study was approved by the Institutional Review Board of Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea (No. KC21RISI0373), and informed consent for an observational study was waived by our institutional policy.
Statistical analyses
Statistical analysis was performed using IBM SPSS Statistics ver. 24.0 (IBM Corp., Armonk, NY, USA). Fisher exact test was used for categorical data, and the Mann-Whitney U-test was used for continuous data. All analyses were based on available data. Significant associations obtained on univariate analysis were used in a multivariate logistic regression analysis to identify independent predictors of high CCI. Statistical significance was set at P<0.05.
RESULTS
The patients’ baseline characteristics were analyzed for 237 patients in YG (≤ 70 years old) and 98 patients in OG (> 70 years old) (Table 2). Body mass index (BMI) was significantly higher in YG (24.1±3.3 vs. 22.9±3.2, P=0.003) and smoking was significantly higher in YG (75 [31.6%] vs. 14 [14.3%]; P=0.001). Patients with underlying diseases such as hypertension, diabetes, cardiovascular disease, and chronic obstructive pulmonary disease (COPD) were significantly higher in the OG group. The proportion of patients with the American Society of Anesthesiologists (ASA) physical status (PS) classification of ≥ III was higher in the OG group, but the difference was not statistically significant. There were no differences in tumor location, type of surgery, and preoperative C-reactive protein (CRP) levels between the 2 groups.
Despite the poorer baseline characteristics of OG, the perioperative outcomes were similar (Table 3). The operation time was longer in the YG group (215±100.6 minutes vs. 189±88.4 minutes, P=0.023). Pathological stage, transfusion rate, and postoperative day (POD) 3 to 4 CRP levels were not different between the groups. Median length of hospital stays (YG, 5 days vs. OG, 5 days; P=0.320) and readmission rates (YG, 18 [7.6%] vs. OG, 4 [4.1%]; P=0.238) did not differ between the groups.
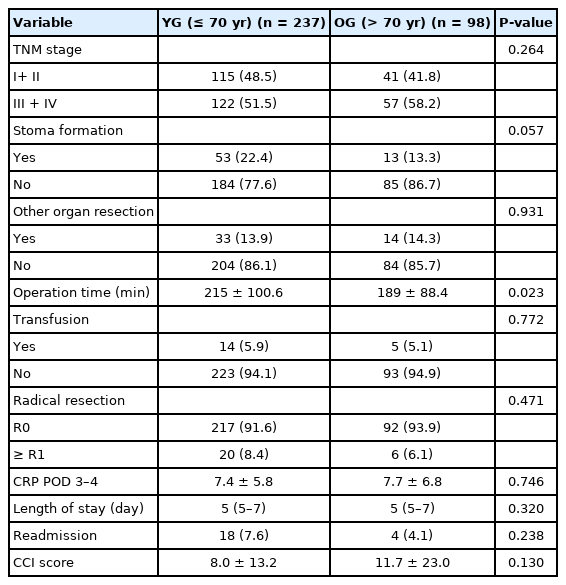
Pathologic and perioperative outcomes
In total, 116 patients (34.6%) developed postoperative complications. The most common complications were wound complications (7.8%) and ileus (7.2%). When comparing tumor location, rectal cancer patients showed significantly higher complications rate (52.1% vs. 27.6%, P<0.001). All of the complication details were described in Supplementary Table 1. The mean CCI for the whole group was 9.1±16.7. There was no significant difference in CCI score between both groups (YG, 8.0±13.2 vs. OG, 11.7±23.0; P=0.130).
The number of patients with low CCI (< 26.2) was 297 (88.7%), and 38 (11.3%) had a high CCI (≥ 26.2). In regression analysis, the old age (> 70 years) was not a risk factor to high CCI in all patients (odds ratio [OR], 1.297; 95% confidence interval [CI], 0.634–2.653; P=0.477) (Tables 4, 5). Subgroup analysis was performed to evaluate the predictive factors of high CCI in each group. In multivariate analysis, high BMI (OR, 3.151; 95% CI, 1.199–8.276, P=0.020) and colon obstruction (OR, 4.159; 95% CI, 1.429–12.107; P=0.009) were strong predictive factors for high CCI in YG. However, in OG, CRP level on POD 3 to 4 (OR, 6.079; 95% CI, 1.117–33.076; P=0.037) was the only strong predictive factor for high CCI.

Univariate regression analysis for predicting high comprehensive complication index
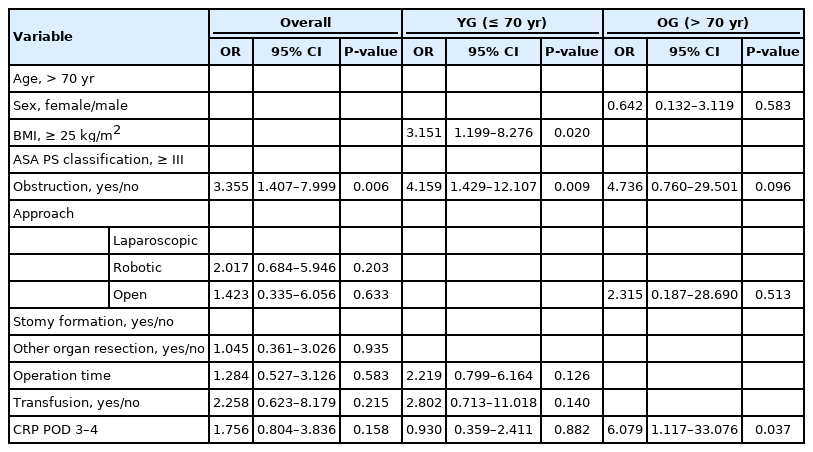
Multivariate regression analysis for predicting high comprehensive complication index
DISCUSSION
The population is rapidly aging in the Republic of Korea [15]. Old age, tends to have comorbidities and frailty issues, is associated with increased postoperative complications in patients with gastrointestinal malignancies [16, 17]. According to literature, early complications after colorectal cancer surgery were seen in 19% to 40% of patients [18, 19]. In this study, overall postoperative complications were seen in 116 patients (34.6%), and when comparing the 2 groups, YG had 83 patients (35.0%), and OG had 33 patients (33.7%) (P=0.900). These results were similar to those of a previous study. There was no significant difference between the 2 groups when comparing complications using the CCI (YG, 8.0±13.2 vs. OG, 11.7±23.0; P=0.130). There was no statistical difference in the duration of hospital stay between the 2 groups (YG, 5 days vs. OG, 5 days; P=0.320).
Our study validated the clinical usefulness of the ERAS protocol in elderly patients with colorectal cancer. OG patients had poorer baseline characteristics, such as a high prevalence of comorbidities (hypertension, diabetes, cardiovascular disease, and COPD) and a high proportion of patients with ASA PS classification of ≥ III (Table 2). Despite having more vulnerable factors, the perioperative outcomes were not inferior to those of YG. Several evidence-based studies have demonstrated the ERAS protocol to support body recovery by reducing the stress response during surgery [20]. This finding implies that the ERAS protocol is safe and feasible in elderly patients, and reduction in surgical stress is especially important for elderly patients with many comorbidities and frailties.
Subgroup analysis was performed to determine the factors that influence high morbidity in each group. In multivariable analysis, high BMI and obstructive colon cancer were strong predictive factors for high CCI in the YG. According to many studies, a high BMI (≥ 30 kg/m2) is highly associated with increased postoperative morbidity, especially surgical site infections [21, 22]. Additionally, obstructive colon cancer has been identified as a risk factor for increased complications [23, 24]. Colon obstruction causes loss of electrolyte and water, often infection, and impedes blood flow to the intestine [25]. Patients with a high BMI or obstructive colon cancer need to be treated more carefully.
CRP is a well-known acute-phase biomarker that can indicate surgical complications [26]. It reached a peak level in the plasma after 48 hours. It can also be used as a marker for infectious complications after surgery. CRP levels were the most accurate on POD 4. In multivariate analysis, OG showed that high CRP (≥ 6.47 mg/dL) on POD 3 to 4 was a significant predictor of severe complications (OR, 6.079; 95% CI, 1.117–33.076; P=0.037). The optimal cutoff value of postoperative CRP was determined by receiver operating characteristic curve analysis. If the CRP level is high on POD 3 or 4, it can be used as a safety index to postpone discharge in elderly patients using the ERAS protocol.
The definition of the elderly varies for each literature, from 65 to 80 years old [9, 27]. Based on an Italian study [28] that applied the ERAS protocol to high-risk patients and a study to determine the cutoff age related to colorectal cancer-specific survival [29], this study defined the elderly based on the age of 70 years.
This study has several limitations. First, this was a retrospective study. Due to the retrospective design, there was potential bias and missing data in the medical records. Compliance data were not checked thoroughly because it was in the early phase of implementing the ERAS protocol at our institution. Data were not shown due to insufficiency, however, preliminary results showed high compliance rates in both groups (Supplementary Table 2). Future large-scale studies are needed to validate the results of this study. Currently, ERAS protocol items have been added and changed at our institution. Epidural anesthesia was excluded, the surgical drain and urinary catheter were removed earlier, and the oral intake schedule was changed. Further studies are needed to evaluate the differences in the results based on these changes.
In conclusion, age does not affect surgical outcomes in patients with colorectal cancer using the ERAS protocol. Implementing the ERAS protocol in patients aged > 70 years is safe and feasible without an increase in complications or readmission rates compared to young patients.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
SUPPLEMENTARY MATERIALS
Supplementary materials for this study are presented online (available at https://doi.org/10.3393/ac.2021.00283.0040).
Supplementary Table 1. Complications in colorectal cancer surgery
Supplementary Table 2. Enhanced recovery after surgery (ERAS) compliance