Single-port robot-assisted abdominoperineal resection: a case review of the first four experiences
Article information

Abstract
Recently, abdominoperineal resection (APR) using a robot has been demonstrated in other studies. However, there has been no report on APR for rectal cancer using the single-port robot (SPR) platform. In response to this research gap, we described the clinical experience of APR using a SPR. From April 2019 to March 2020, APR using a SPR platform was performed in a total of 4 patients. Three patients had a transumbilical approach, and 1 patient had a transstoma site approach. The average operation time was 307 minutes, and the patient docking time to the SPR platform was 133.5 minutes. There were no complications during the operation, and no laparoscopy or open conversion. No reoperation occurred within 30 days. Mild postoperative complications occurred in 2 patients. We found that APR has safety and feasibility in surgery using an SPR platform. There was no intraoperative event and severe postoperative complications.
INTRODUCTION
Since laparoscopic surgery for colorectal cancer was introduced in the 1990s, treatment for colorectal cancer has been evolving. Surgical methods for colorectal cancer have been diversified into multiport laparoscopic surgery as well as single-port laparoscopic surgery [1, 2]. Accordingly, performance of colorectal cancer surgery using an open approach technique is decreasing [3, 4]. This is because many benefits can be obtained when performing laparoscopic surgery, including reduced patient pain, less infection at the surgical site, less analgesic use, and no difference in oncologic outcome [5].
Recently, new developments have been realized with the introduction of robotic surgery. In addition, studies have reported that robot-assisted colorectal cancer surgery has no significant difference in oncologic outcome compared to laparoscopic surgery [6, 7]. However, studies on abdominoperineal resection (APR) using robots in primary rectal malignancy are limited [8]. Research on long-term outcomes according to robotic surgery is insufficient, and studies comparing robotic surgery and conventional laparoscopic surgery are insufficient. In addition to these points, current robot surgery has a disadvantage in that it requires 5 to 6 ports [9]. Moreover, as the length of the main wound for delivery of the specimen increases, the incision length also increases. Eventually, the number and size of wounds increase, which increases the patient burden. In response, colorectal cancer surgery using a single-port robot (SPR) was developed [10]. Using one port, it is possible not only to reduce the wound load of the patient but also to reduce pain and improve cosmetics.
The possibility of APR using a robot has been demonstrated in other studies [8]. However, there has been no report on APR for rectal cancer using the SPR platform. As a result, we described the clinical experience of APR using an SPR.
TECHNIQUE
Ethical statements
This study was conducted according to the Declarations of Helsinki with ethical approval obtained from the Institutional Review Board of Samsung Medical Center in Seoul, Korea (No. 2020-09-179-005). The requirement for informed consent was waived because of the retrospective nature of the study.
Surgical technique
All patients were treated with neoadjuvant chemoradiotherapy with clinically defined node metastasis in T3 cancer and received surgery 8 to 12 weeks after the end of radiotherapy. The patients were admitted 2 days before surgery; from the day before surgery, mechanical bowel preparation was performed with an agent containing magnesium oxide, sodium picosulfate, and citric acid hydrate as the main components. General anesthesia was administered, and the patient was placed in a lithotomy position. Before surgery, pre-stoma was marked on the abdomen where the stoma was expected to form.
Using a transumbilical approach, a docking system was formed using a medium-size wound protector and a handmade glove port after a 4-cm incision around the umbilicus. An additional 12-mm trocar was inserted into the right lower abdominal quadrant (Fig. 1A). When approaching through the stoma site, a circular incision of 2.5 cm in diameter was applied to the left lower quadrant of the abdomen, and a docking system was formed using a wound protector and a handmade glove port (Figs. 1B, 2). An SPR docking trocar and 12-mm trocar were applied to the handmade glove port. Before docking the robot, the patient’s bed was placed in the Trendelenburg position with right-side tilt.
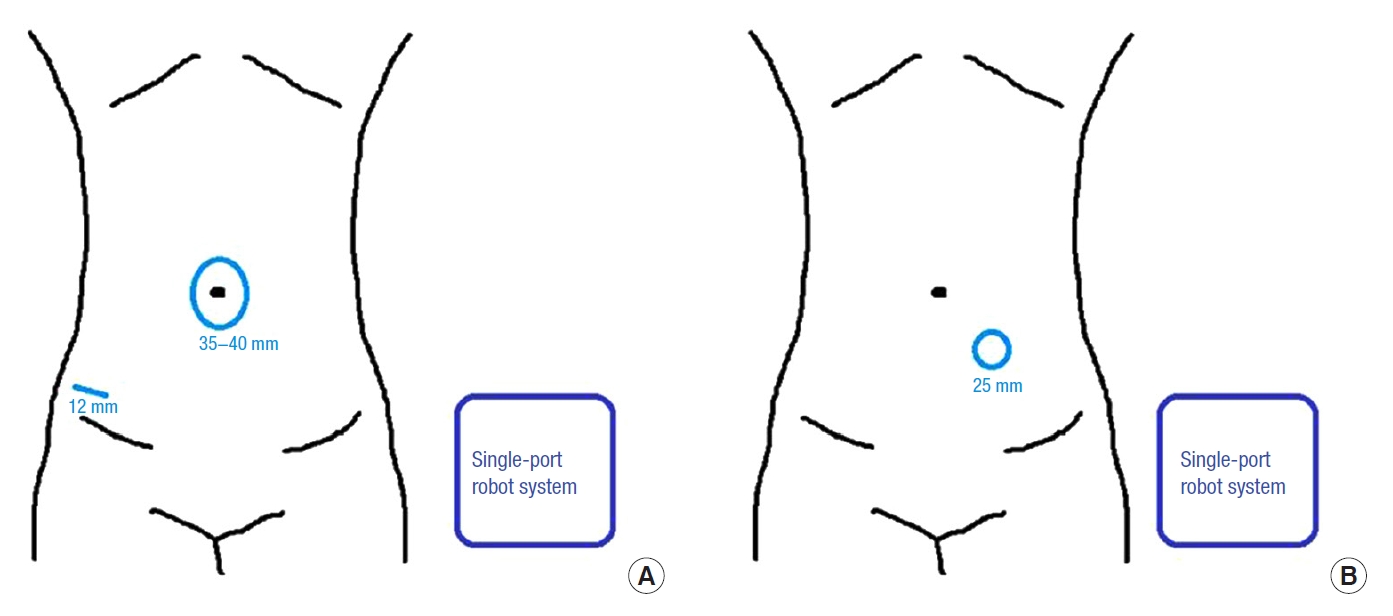
Incision site and length of single-port robot system. (A) Transumbilical incision site. (B) Transstoma site.
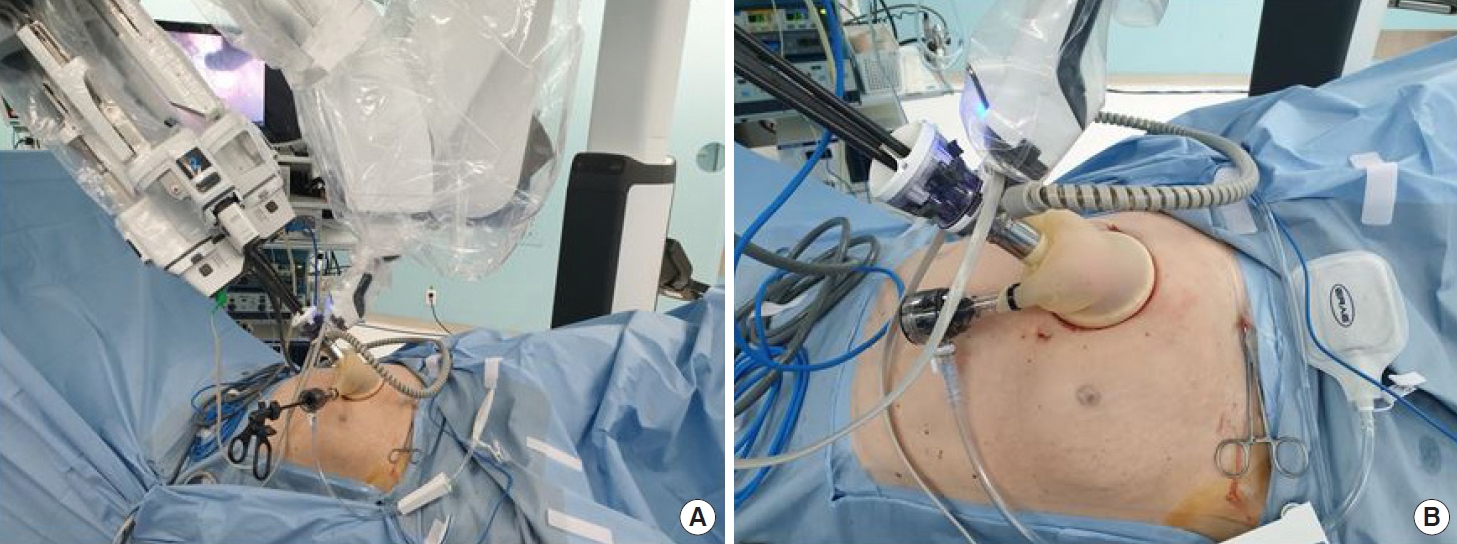
Single-port robot system in a left-side stoma site docking state. (A) Full view of docking on robot. (B) Close-up view of docking on robot.
After docking the robot, the abdomen was inflated with CO2 gas, and the robot arms were inserted into the abdominal cavity. Next, the fat around the inferior mesenteric artery was identified by dissection. Subsequently, the artery was resected after ligation at 1 cm above the base using an endoscopic clip (Hem-o-lok, Weck Surgical Instruments, Teleflex Medical, Durham, NC, USA). Moving upward again, the inferior mesenteric vein was ligated, and medial to lateral dissection was performed. Subsequently, the sigmoid colon was mobilized from the lateral side and dissected to the splenic flexure.
In female patients, before total mesorectal excision (TME), the uterus was pulled toward the peritoneum of the anterior side using a surgical straight needle to secure the field of view (Fig. 3A). When performing TME, sigmoid colon traction was performed with a non-traumatic grasper through a 12-mm trocar of the glove port. Dissection of the mesorectum was performed until the levator ani muscle was revealed. The anterior side was dissected, including Denonvilliers’ fascia. When the sigmoid colon was long or the pelvis was narrow and deep, the proximal end of specimen was resected using the Signia stapling system 60 (Medtronic Ltd., Minneapolis, MN, USA) (Fig. 3B). After entering the stapler into the abdominal cavity through the 12-mm port or additional port, the proximal end was resected. However, when the pelvis was wide and shallow, specimens were delivered by perineal approach after dissection of mesorectal fascia.
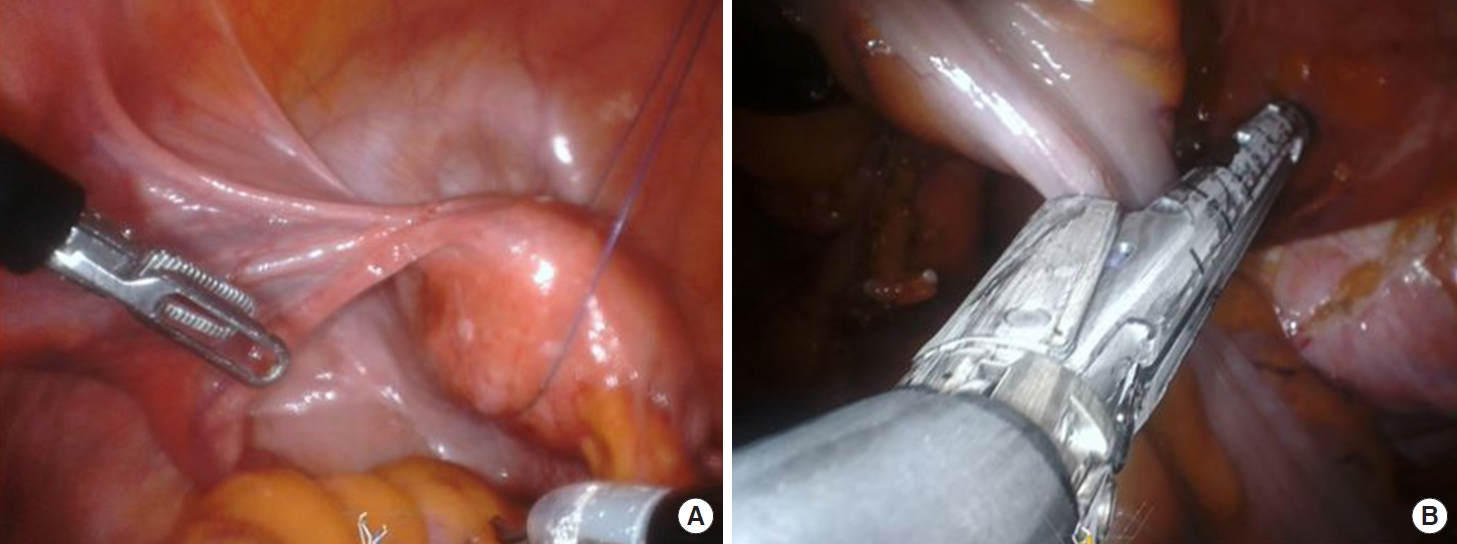
Intraabdominal technique of single-port robot surgery. (A) Uterus suspension on anterior pelvic peritoneum by surgical straight needle. (B) Proximal end resection using a linear stapling Signia stapling system (Medtronic Ltd., Minneapolis, MN, USA).
The specimen was removed through a perineal wound, and the proximal end was removed with sufficient margin. Subsequently, the perineum wound was sealed at each layer. The camera was inserted through the stoma site, the end of the resected colon was excised and fixed to the fascia, and stoma maturation was performed. In patients with a transumbilical incision, stoma maturation was performed after suturing the fascia of the umbilicus incision site in a layer-by-layer fashion. In wounds with umbilicus and additional trocars, the skin was sutured using 4-0 Monosyn and sealed using a skin adhesive agent (Dermabond Advanced Topical Skin Adhesive, Ethicon, Cincinnati, OH, USA).
Results
From April 2019 to March 2020, APR using an SPR platform was performed in 4 patients. The patients were 2 males and 2 females, with an average body mass index of 23.02 kg/m2, and an average age of 60.25 years (range, 50–74 years). The tumor location in 2 patients was a distance of 2 cm from the anal verge, 1 patient at 1 cm, and 1 patient at 0.5 cm. All patients underwent preoperative colonoscopy, abdominopelvic computed tomography (CT), chest CT, and rectal magnetic resonance imaging. Patients were diagnosed with clinical T3 low rectal cancer; 3 patients were diagnosed with adenocarcinoma in colonoscopy biopsy before surgery, and 1 patient was diagnosed with signet ring cell carcinoma. Patients underwent neoadjuvant chemoradiotherapy with capecitabine (Xeloda, Hoffman-LaRoche, Nutley, NJ, USA) before surgery. All patients received sufficient information and agreed to the surgery using an SPR platform before surgery. Patient characteristics are given in Table 1.

Characteristics of patients with single-port robot abdominoperineal resection
The average operation time was 307 minutes, and the robot docking time of the SPR platform was 133.5 minutes. The average estimated blood loss was 132.5 mL. As additional surgery was performed in 3 patients, there was a difference between operation time and docking time. There were no complications during the operation and no laparoscopy or open conversion. No reoperation occurred within 30 days.
The first bowel movement through the patient’s end colostomy was confirmed on the second postoperative day (POD). The day after surgery, sips of water were allowed; a soft, bland diet was provided from POD 2. During hospitalization, all patients were trained to use a stoma. Postoperative complications occurred in 2 patients. In both patients, urinary retention occurred on POD 4. No other complications occurred. Patient clinicopathologic data and postoperative data are given in Table 2.

Clinicopathologic and postoperative data of single-port robot abdominoperineal resection
The average mass size on pathological examination was 4.35 cm (range, 2.5–5.2 cm). The average length of the safety resection margin from the tumor was 17.7 cm (range, 9–40 cm) for the proximal and 3.4 cm (range, 1.4–5.0 cm) for the distal margin. No cancer cells were found in the proximal or distal margin. One patient had a positive circumferential margin. An average of 17.8 (range, 9–26) regional lymph nodes (LNs) was harvested, and 2 and 4 LN metastases were identified in 2 patients, respectively. All patients underwent TME. The postoperative stage was confirmed as IIA in 2 patients (pathologic [p]T3N0M0), IVA in 1 patient (pT3N1bM1a), and IIIB in 1 patient (pT3N2aM0).
DISCUSSION
As minimally invasive surgery develops, new types of surgery are advancing. Laparoscopic surgery using single-port rather than general laparoscopic surgery was introduced [11-13]. Knowledge of the benefits of reduced wound length with laparoscopic surgery continued to motivate new surgical methods. Of these, continuous research has been conducted on laparoscopic surgery with only 1 port, and single-incision laparoscopic surgery has been published. By reducing the size and number of surgical wounds to patients, there are advantages such as pain reduction, cosmetic advantage, and rapid postoperative recovery [11]. In addition, there is an advantage of shortening hospital stay length by reducing the probability of surgical site infection or hernia after surgery. Moreover, in surgery to create permanent stoma such as APR, the number of wounds can be reduced using a predetermined incision site [2]. The presented APR surgery using an SPR through the colostomy site is an extension of the single-port laparoscopic reference through a previously developed colostomy site.
In 2018, an SPR platform was developed by Intuitive Surgical (Sunnyvale, CA, USA). Since this platform was introduced, robotic surgery has been advanced in various fields. Recently, as prostatectomy using an SPR has been performed and safety has been demonstrated continuously, attempts at colorectal surgery have begun [14]. Samsung Medical Center introduced the SPR platform in April 2019, and surgery for colorectal cancer patients began. Through several surgeries using the SPR platform, we analyzed the patient group suitable for the SPR platform and analyzed those who were suitable for APR using the colostomy site. APR was developed in 4 patients, and there was no severe postoperative complication or reoperation following surgery. Only mild complications occurred.
APR using the SPR platform is feasible and safe. Nevertheless, APR using SPR is more difficult than standard robot-assisted APR. There are many considerations, from dissection of the mesorectum to access to the main mass and delivery of the specimen. Recently, as laparoscopic devices have been developed, energy devices or endo staplers have been developed; but there are no products available for the SPR platform, which increases the surgical difficulty. In our results, sufficient mesorectum was dissected during surgery, but the number of harvested LNs varied from 9 to 26. In the SPR platform, deliberation should be given to the location when harvesting LN and areas requiring additional dissection. Additional considerations are needed for the circumferential margin of positive results in one patient. In addition, through the study on the patient’s pain after surgery and the frequency of analgesic agent use, it is necessary to confirm the pain relief effect in later studies. Finally, there are no oncological outcomes in colorectal cancer for the SPR surgery technique. Future follow-up is needed to compare with conventional robot operation.
Already, single-incision laparoscopic APR is widely performed. However, we tried APR using SPR. When using SPR, there are several advantages compared to the previous single-incision laparoscopic APR. First, an extended three-dimensional view can be provided when the operator tries to TME. Second, the operator’s fatigue due to surgery is not high enough than laparoscopic surgery. Third, it does not require the assistance of an experienced scopist. Lastly, there is no tremor when using the robot arm. It is necessary to check what advantages and disadvantages there are in the future.
In conclusion, we found that APR has safety and feasibility in surgery using an SPR platform. No notable intraoperative event occurred in the 4 patients who underwent surgery. However, further development of surgical techniques and instrument development is needed. In addition, there is a need for research on the additional advantages of rectal cancer in comparison with conventional robot operation.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.