Benefits and risks of diverting stoma creation during rectal cancer surgery
Article information

Abstract
Purpose
A consensus has been reached regarding diverting stoma (DS) construction in rectal cancer surgery to avoid reoperation related to anastomotic leakage. However, the incidence of stoma-related complications (SRCs) remains high. In this study, we examined the perioperative outcomes of DS construction in patients who underwent sphincter-preserving surgery for rectal cancer.
Methods
We included 400 participants who underwent radical sphincter-preserving surgery for rectal cancer between 2005 and 2017. These participants were divided into the DS (+) and DS (–) groups, and the outcomes, including postoperative complications, were compared.
Results
The incidence of ileus was higher in the DS (+) group than in the DS (–) group (P<0.01); however, no patients in the DS (+) group showed grade 3 anastomotic leakage. Furthermore, early SRCs were observed in 33 patients (21.6%) and bowel obstruction-related stoma outlet syndrome occurred in 19 patients (12.4%). There was no significant intergroup difference in the incidence of grade 3b postoperative complications. However, the most common reason for reoperation was different in the 2 groups: anastomotic leakage in 91.7% of patients with grade 3b postoperative complications in the DS (–) group, and SRCs in 85.7% of patients with grade 3b postoperative complications in the DS (+) group.
Conclusion
Patients with DS showed higher incidence rates of overall postoperative complications, severe postoperative complications (grade 3), and bowel obstruction, including stoma outlet syndrome, than patients without DS. Therefore, it is important to construct an appropriate DS to avoid SRCs and to be more selective in assigning patients for DS construction.
INTRODUCTION
In recent years, the development of surgical instruments and operation techniques for lower rectal cancer surgery has led to sphincter preservation [1]. Consequently, the number of cases requiring diverting stoma (DS) creation has increased. A consensus was reached regarding DS construction during rectal cancer surgery to prevent severe peritonitis related to anastomotic leakage [2-5]. Anastomotic leakage significantly reduces patients’ quality of life (QOL); therefore, the prevention of anastomotic leakage-related severe peritonitis is crucial. Moreover, stoma-related complications (SRCs) can reduce patients’ QOL. Numerous studies have reported the incidence of SRCs to be between 21% and 70% [6, 7]. The onset rate of SRCs reported by different studies varies greatly, and relatively few cases have been reported. Whether the benefits of DS construction outweigh the effects of SRCs remains unelucidated.
We retrospectively compared the short-term outcomes of sphincter-preserving surgery for rectal cancer in patients managed with and without DS.
METHODS
The study design of this retrospective study was approved by the Institutional Review Board of Juntendo University (No. 14-172), and the requirement for patient consent was waived. All methods were performed in accordance with the relevant guidelines and regulations.
We retrospectively enrolled 400 participants who underwent radical sphincter-preserving surgery for rectal cancer between 2005 and 2017. We excluded patients who underwent emergency surgery, transanal ileus tube insertion, or colonic stent placement for obstructive colorectal cancer. DS construction was indicated in patients whose lower tumor margin was ≤ 5 cm from the anus, those receiving preoperative treatment (chemoradiotherapy [CRT] or neoadjuvant chemotherapy [NAC]), those with malnutrition, those on steroid therapy, and those with anastomotic leakage on intraoperative examination. However, surgeons were responsible for the final decision on DS construction.
In cases with a possibility of stoma construction, a stoma site is marked beforehand. A circular skin incision is cut (about 3 cm in diameter) in the corresponding location. The rectus abdominis anterior sheath is cut in the lengthwise direction, and the rectus abdominis muscle is split. We construct a tunnel where 2 fingers enter the intraperitoneal cavity to a sufficient degree. The terminal ileum or transverse colon is selected as a stoma, and a loop stoma is constructed. The oral side is twisted caudally as much as possible. When the ileum is selected as a stoma, we use the ileum from the ileocecal valve (around 30–40 cm).
The participants were divided into the DS (–) and DS (+) groups. Intergroup comparisons were made according to the patient’s background (age, sex, body mass index [BMI], tumor location, CRT or NAC use, and pathological stage), perioperative factors (procedure type, use of lateral lymph node dissection, surgical approach, operative time, volume of intraoperative blood loss, and ano-anastomotic distance [measured intraoperatively using an endoscope]), and postoperative course (interval until the start of oral ingestion, postoperative hospitalization period, postoperative complications, and reoperation). With respect to tumor location, the rectum was classified into the rectosigmoid (RS), upper rectum (Ra), and lower rectum (Rb) [8]. Cancer staging was undertaken using the eighth edition of the American Joint Committee on Cancer, the TNM staging system, and the 2017 World Health Organization classification [9]. Postoperative complications were examined using Common Terminology Criteria for Adverse Events (CTCAE ver. 4.0; National Cancer Institute, Bethesda, MD, USA) [10]. Furthermore, patients with intestinal obstruction related to stenosis of the DS excretory pore were considered to have stoma outlet syndrome. Among postoperative complications, this syndrome was analyzed as a type of bowel obstruction, and infection-related stoma separation was analyzed as a type of surgical site infection (SSI).
SRCs were investigated in the DS (+) group, and the SRCs that developed within 30 days post-surgery were defined as early complications. SRCs were also examined in patients who underwent reoperation, those with a prolonged time to DS reversal, and those in whom DS reversal was impossible.
For statistical analysis, the chi-square test and Fisher exact test were used to compare categorical variables, whereas the Student t-test was used to compare continuous variables. A P-value of 0.05 was considered to indicate statistical significance. We used JMP ver. 10 software (SAS Institute., Cary, NC, USA) for statistical analyses.
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
RESULTS
Patient background
Table 1 shows the patients’ backgrounds. The median patient age was 64 years (range, 25–86 years). The participants consisted of 267 men and 133 women patients. The median BMI of the patients was 23.0 kg/m2 (range, 14.3–34.4 kg/m2). The tumors were located in the RS, Ra, and Rb in 115, 172, and 112 patients, respectively. The laparoscopic approach was adopted in 272 patients (68%). Concerning the surgical procedure, low anterior resection, high anterior resection, and intersphincteric resection were performed in 308 (77.0%), 55 (13.8%), and 37 patients (9.3%), respectively. Furthermore, a DS was constructed in 153 patients (38.3%). Overall, postoperative complications were identified in 120 patients (30.0%), leading to reoperation in 19 patients (4.8%). One case of patient death was recorded due to cerebral hemorrhage.

Baseline characteristics of the patients
Patient characteristics
The characteristics of patients in the DS (–) and DS (+) groups are shown in Table 2. There were no significant intergroup differences in age, sex, or BMI. Regarding the distribution of tumor location, the proportion of patients with Rb tumors was significantly higher in the DS (+) group (P< 0.01). The choice of preoperative treatment, including CRT and NAC, was significantly different in the 2 groups (P< 0.01). The pathologic stage was I, II, III, and IV in 67, 65, 85, and 18 patients in the DS (–) group, and 62, 39, 45, and 7 patients in the DS (+) group, respectively (P= 0.030).
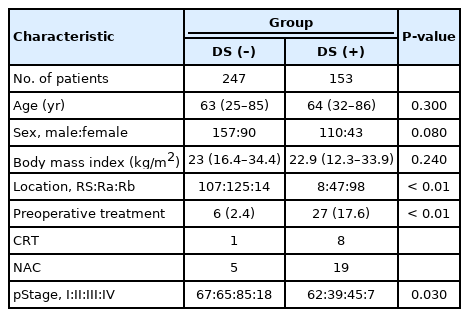
Characteristics of patients in each group
Surgical outcomes
The surgical outcomes of patients in the DS (–) and DS (+) groups are shown in Table 3. There were intergroup differences in the distribution of surgical procedure type, the performance rate of lateral lymph node dissection, and laparoscopic approach rate. The operative time was significantly longer in patients in the DS (+) group (268 minutes vs. 405 minutes, P< 0.01); nonetheless, the volume of blood loss was not significantly different (30 mL vs. 50 mL, P = 0.840). Furthermore, the ano-anastomotic distance was significantly smaller in patients in the DS (+) group (8 cm vs. 4 cm, P< 0.01).
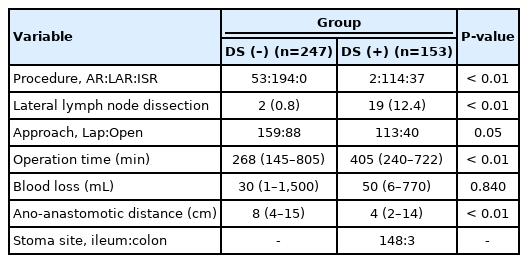
Surgical outcome
Postoperative outcomes
The short-term outcomes of DS construction are shown in Table 4. Oral ingestion was started on postoperative day 6 (range, 4–41) in the DS (–) group and on postoperative day 4 (range, 2–18) in the DS (+) group. This demonstrated that the time to oral ingestion was significantly shorter in the DS (+) group (P= 0.010).

Short-term outcomes
Postoperative complications of grade > 4 were detected in 1 patient in the DS (+) group. Moreover, the number of patients with grade 1-3 postoperative complications was significantly higher in the DS (+) group. However, there was no significant intergroup difference in the number of patients with postoperative complications of grade 3b (12 vs. 7, P= 0.900). There was no significant intergroup difference in the proportion of patients with anastomotic leakage of all grades (10.9% vs. 15.0%, P= 0.310). However, the proportion of patients with anastomotic leakage grade 3b was significantly higher in the DS (–) group (4.5% vs. 0%, P= 0.010). In contrast, regarding bowel obstruction, the incidence of all grades and grade 3 was significantly higher in the DS (+) group (4.0% vs. 25.5%, P< 0.01; 2.4% vs. 17.0%, P< 0.01, respectively).
However, there were no significant intergroup differences in the incidence of SSI and micturition disorders. The postoperative hospitalization period was significantly shorter in the DS (–) group (12 days vs. 15 days, P= 0.020).
Reoperation was required in 12 (4.9%) and 7 patients (4.6%) in the DS (–) and DS (+) groups, respectively, which was not significantly different between the groups (P= 0.900). The reasons for reoperation in the DS (–) group included anastomotic leakage (11 cases) and adhesive bowel obstruction (1 case). In the DS (+) group, the reasons for reoperation included stoma outlet syndrome (4 cases), electrolyte imbalance (1 case), mucocutaneous stoma separation (1 case), and intraperitoneal hematoma (1 case); moreover, reoperation was required for SRCs in 6 of the 7 patients (Table 5).
Stoma-related complications
The median follow-up time after DS construction was 229 days (range, 10–2,331 days). In 145 of the 153 patients (94.8%), DS reversal was achieved. In 8 patients (5.2%), a DS was left due to death caused by another disease (3 cases), refractory fistulae (2 cases), stage IV cancer (2 cases), and the patient’s request (1 case).
Stoma-related complications
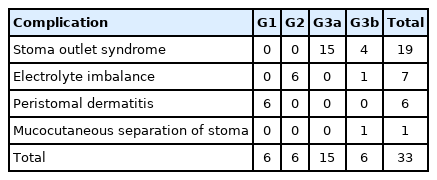
Early complications were observed in 33 patients (21.6%): stoma outlet syndrome (19 cases, 12.4%), electrolyte imbalance (7 cases, 4.6%), peristomal dermatitis (6 cases, 3.9%), and infection-related stoma separation (1 case, 0.7%). Neither hemorrhage nor necrosis was reported in these patients (Table 5). As a late complication, parastomal hernia was noted in 3 patients (2.0%). Neither prolapse nor fistula formation was noted.
DISCUSSION
Sphincter-preserving surgery is selected for patients with lower rectal cancer due to recent advances in the use of automatic staplers and the broad indications for laparoscopic or robotic surgery. Consequently, DS construction is being performed in an increasing number of patients. Furthermore, advances in preoperative treatment (CRT and NAC) might also have accelerated the increase in the number of DS construction procedures, considering an adverse reaction-related delay in wound healing. The incidence of SRCs was previously reported to be between 21% and 70% [6, 7, 11].
In this study, DS construction was also frequently selected for patients with advanced lower rectal tumors who underwent preoperative treatment or in whom lateral lymph node dissection was simultaneously scheduled. This might have depended on the tumor location and oncological factors.
In previous studies, DS construction in sphincter-preserving surgery for rectal cancer reduced the risk of severe peritonitis related to anastomotic leakage [7, 12, 13]. However, there is no precise method of identifying which patients will benefit from a DS. In our study, although the incidence of overall anastomotic leakage was similar in patients with and without DS, the incidence of severe anastomotic leakage (grade 3) was significantly higher in patients without DS. These results were favorable, similar to the results of previous studies, and DS construction was considered to be worthwhile.
Conversely, patients with DS were more likely to develop postoperative complications, which were categorized according to the overall grade. The incidence of ileus, which was categorized in both grades 2 and 3, was significantly higher in patients with DS. These findings are thought to have been related to the additional procedure of stoma construction. Furthermore, diverting loop ileostomy construction (96.7%) was more frequently performed than loop colostomy, and stoma outlet syndrome occurred in 19 of 33 patients (57.6%) with SRCs. Fujii et al. [14] reported that adhesions and twisting of the ileostomy were the causes of stoma outlet obstruction, and loop ileostomy was reported as an independent risk factor for stoma outlet syndrome [15].
The postoperative hospitalization period was significantly longer in patients in the DS (+) group. First, it should be initially considered that patients with all grades of bowel obstruction, including stoma outlet syndrome, were more common in the DS (+) group. Once bowel obstruction occurred, hospitalization might have been prolonged by intestinal peristalsis and interruption of oral intake, even though the patients were conservatively treated with ileus tube insertion or tubing of the DS afferent loop. Second, patients and families require time to learn about stoma management during hospitalization. Cirocchi et al. [16] also reported similar results. However, Hignett et al. [17] noted no prolongation of the admission period. These differences might have also been associated with the patients’ background or region.
There was no significant intergroup difference in the number of reoperations. In the DS (+) group, no patient required reoperation due to anastomotic leakage, which aligns with the findings of Shiomi et al. [12]. However, reoperation related to SRCs was required in our study. In addition, anastomotic leakage was a reason for reoperation in 11 of 12 patients (91.7%) in the DS (–) group, whereas reoperations related to SRCs accounted for 85.7% (n= 6) of the 7 patients in the DS (+) group. In patients with SRCs, the anastomosis was confirmed prior to reoperation. Four cases with anastomotic leakage necessitated DS reconstruction. Three patients without anastomotic leakage underwent DS closure.
In our study, stoma outlet syndrome improved in 80% of patients after conservative treatment, such as tube placement, and this was the most common SRC. However, 4 patients required reoperation. The use of an operation technique that does not cause stoma outlet syndrome is crucial. We had a case wherein a patient was reoperated using several devices for DS construction, which is one of the limitations of our study. Furthermore, we introduced other articles or devices used for DS creation. It was reported that stoma outlet syndrome could be prevented by avoiding twists during intestinal elevation, ameliorating stoma construction procedures such as the angle of approaching the abdominal wall or handling subcutaneous fat thickness, or applying a DS for cases involving the colon [11, 14]. Furthermore, it may be important to perform DS with a change of the elevated intestinal tract while considering methods other than the use of a DS and aspects of patients’ background, such as age [18-20].
DS reversal was impossible in 8 patients (5.2%) in this study. Gadan et al. [21] reported a reversal impossibility rate of 18.2% (20 of 110 cases). The DS reversal rate in our study was higher than that reported in their study; however, DS reversal was achieved within 6 months after surgery in 55 patients (35.9%) and ≥ 2 years after surgery in many patients. This was possibly due to the follow-up period and because the opinions of the attending physicians regarding DS reversal were not standardized in the initial follow-up phase. DS reversal after treatment was expected in patients who underwent adjuvant chemotherapy.
This study has some limitations. First, we included a small number of cases, and the patients were from a single racial group. Moreover, we conducted a retrospective, single-center study. The DS procedure gradually changed over time. For example, DS was created in the ileum of the distal part from the ileocecal valve (about 40–50 cm), and the oral side of the intestinal tract was lifted into a more natural position without being concerned with the caudal side. Finally, after reobservation, we confirmed that there was no torsion of the DS. Therefore, it is necessary to conduct a prospective study with a large number of cases wherein standardized DS indications and procedures are used.
In rectal cancer surgery, the use of a DS helped prevent severe peritonitis related to anastomotic leakage and led to an early start of oral ingestion; nonetheless, it did not reduce the postoperative hospitalization period. Furthermore, postoperative complications included an increase in the incidence of bowel obstruction, including stoma outlet syndrome, in patients in the DS (+) group, and SRC-related reoperation was required in some patients. Therefore, it is important to construct an appropriate DS to avoid SRCs and to select appropriate patients for whom a DS should be constructed.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: MK. Data curation: MK. Formal analysis: MK. Investigation: MK, KH, YO, RT. Methodology: MK, SK, SM, KS, SI. Writing–original draft: MK. Writing–review & editing: KS, MT, YK, YT.
All authors have read and approved the final manuscript.