Puborectalis Muscle Involvement on Magnetic Resonance Imaging in Complex Fistula: A New Perspective on Diagnosis and Treatment
Article information

Abstract
Purpose
According to recent studies, magnetic resonance imaging (MRI) assessment of complex fistulas provides a significant benefit compared to fistulography, computed tomography, and ultrasonography. The aim of this study was to describe the accuracy of MRI and the importance of identifying puborectalis muscle involvement on MRI in patients with complex fistula.
Methods
All patients who were clinically diagnosed with ‘complex’ or showed multiple fistula tracts underwent fistula MRI. Eligible patients were consecutive patients who underwent fistula MRI between September 2018 and September 2019 at our hospital.
Results
A total of 83 patients (74 males, 9 females; 116 tracts) were included in this study. The sensitivity and specificity of MRI in diagnosing fistula tracts were 94.8% and 98.2%, respectively. The sensitivity and specificity in identifying internal opening were 93.9% and 97.3%, respectively. Of the 35 patients with puborectalis muscle involvement in the MRI, 31 images of suprasphincteric-type patients on the Park’s classification were classified. The patients of puborectalis involvement were divided into 2 groups according to the surgical procedure that was performed. There were 12 sphincter-saving procedures and 19 sphincter division procedures performed. Recurrence was seen in 2 patients in the sphincter-saving procedure group, while no case was seen in the sphincter division procedure group. Five complications were found in the sphincter division procedure group, of which 2 reported incontinence.
Conclusion
Fistula MRI is a highly accurate examination for evaluating complex fistulas, and the puborectalis muscle involvement findings are very important for diagnosis and treatment.
INTRODUCTION
The first reports on the accuracy of magnetic resonance imaging (MRI) for the detection and classification of fistulas were published in 1992 and 1994 [1, 2]. Since then, many articles have reported high accuracy values for MRI in the detection of fistula tracts and secondary extensions [3, 4]. Moreover, MRI has been shown to alter the surgical approach and influence surgical outcomes [5-7]. Most importantly, MRI-guided surgery can significantly reduce postoperative recurrence in complex cases by 75% [7]. Agreement for preoperative assessment of perianal fistula using MRI between experts and novices is good, while intraobserver agreement is also acceptable after a period of directed education [8]. Therefore, MRI is identified as the modality of choice for the preoperative evaluation of complex or recurrent fistula [5].
The Standard Practice Task Force, by the American Society of Colon and Rectal Surgeons (ASCRS), classifies anal fistulas as ‘simple’ and ‘complex’. The latter category identifies the increased risk of incontinence after surgery [9]. Parks et al. [10] emphasized the importance of an adequate anorectal angle to maintain continence. The anorectal angle is created by the anterior pull of the puborectalis sling at the level of the anorectal junction. Puborectalis muscle contraction was an independent variable with the strongest correlation to the clinical severity of incontinence [11]. MRI not only shows supralevator extension of the fistula and a rectal opening with high accuracy but also precisely shows puborectalis muscle involvement of the fistula [12]. Therefore, we believe that it is essential to confirm the presence or absence of puborectalis muscle involvement on MRI before operation.
According to recent studies, MRI assessment of complex fistulas provides a significant benefit compared to fistulography, computed tomography (CT), and ultrasonography [5, 13]. Inevitably, the demand for MRI techniques in the treatment of complex fistula will increase. The aim of this study was to describe the accuracy of MRI and the importance of identifying puborectalis muscle involvement on MRI in patients with complex fistula.
METHODS
Patients
This study was approved by the Institutional Review Boards of the participating institutions (No. 2020-004). The requirement for informed consent of patients was waived because of the retrospective nature of the study. Patients referred to the outpatient clinic for anal fistula were assessed for eligibility. The attending surgeon identified potential participants and classified the anal fistula as ‘complex’ or ‘simple’ according to the ASCRS fistula guidelines [14]. All patients who were clinically diagnosed with ‘complex’ or showed multiple fistula tracts underwent fistula MRI. Eligible patients were consecutive patients who underwent fistula MRI between September 2018 and September 2019 at the Seoul Songdo Hospital. Demographic data, medical history, as well as surgical and follow-up details of the patients were recorded. All patients underwent acid-fast bacterium stain of anal discharge and punch biopsies at the external opening sites to exclude tuberculosis or Crohn fistula. All patients underwent anal manometry and pudendal nerve terminal motor latency testing for evaluation of anorectal physiology. Patients without acute anal sepsis (such as abscess) underwent MRI a week before surgery. In the case of acute anal abscess on ultrasound, MRI was performed after adequate drainage for 4 weeks.
Magnetic resonance imaging technique
All MRI examinations were performed in a supine position at rest using a 1.5 T magnet (Intera 1.5 T, Philips, Amsterdam, Netherlands) with a 4-channel phased-array sense body coil. We obtained T2-weighted turbo spin echo (TSE) sagittal, anal axial, anal coronal, and short tau inversion recovery anal axial images with the following imaging parameters: TR/TE effect 600 to 780/20; flip angle, 90°; field of view, 225 to 400 mm; slice thickness, 3 mm interleaved; imaging matrix, 512× 512. After 7.5 mL of contrast material (Gadovist, Bayer Schering Pharma AG, Germany) was injected, fat-saturated T1-weighted TSE magnetic resonance (MR) images (sagittal, anal axial, and anal coronal) were obtained. After the MRI procedure, the source images were electronically transferred to a picture archiving and communication system (Piview STAR, INFINITT Technology, Seoul, Korea).
One experienced radiologist evaluated the MR images using an Easy Vision Workstation (Philips). To characterize an anal fistula, the radiologist analyzed images and described the following: (1) internal opening site, (2) external opening site, (3) existence of rectal opening, (4) demonstration of hidden areas of sepsis and secondary extensions, (5) coexisting fistulas, (6) detailed description of the pathway of the fistulous tract and its relationship with the puborectalis muscle, and (7) classification of the fistula type.
Magnetic resonance imaging accuracy
Intraoperatively, the internal opening was identified by injecting methylene blue solution through the external opening after the intraoperative rectal examination. The findings of clinical examination and MRI finding were correlated with the intraoperative findings. During surgery, the details of the openings and the tracts were carefully noted and then compared to the MRI findings. Any findings missed or misdiagnosed by MRI were carefully noted. These inaccuracies of MRI were then used to calculate sensitivity and specificity of the MRI.
Puborectalis muscle involvement
The MRI of all patients was described by detailed description of the pathway of the fistulous tract and its relationship with the puborectalis muscle by the radiologist. Puborectalis muscle involvement was defined as the case where the fistula tract passed the puborectalis muscle or the end of the fistula was located, or when the associated abscess invaded the puborectalis muscle. The MRI findings of patients with puborectalis muscle involvement in suprasphincteric type on Park’s classification were analyzed. The MRI findings of a total of 31 patients appear as follows: the tract was inflamed into the levator ani muscle (including puborectalis muscle) and then stretched to the supralevator space and ischioanal space (Fig. 1A); the tract passed through the levator ani muscle (including puborectalis muscle) and into the ischioanal space (Fig. 1B); the tract passed through the puborectalis muscle and into the ischioanal space (Fig. 1C); the fistula tract was inflamed into the levator ani muscle (including puborectalis muscle) and was confined to it (Fig. 1D); and the fistula tract was inflamed into the puborectalis muscle and was confined to it (Fig. 1E).
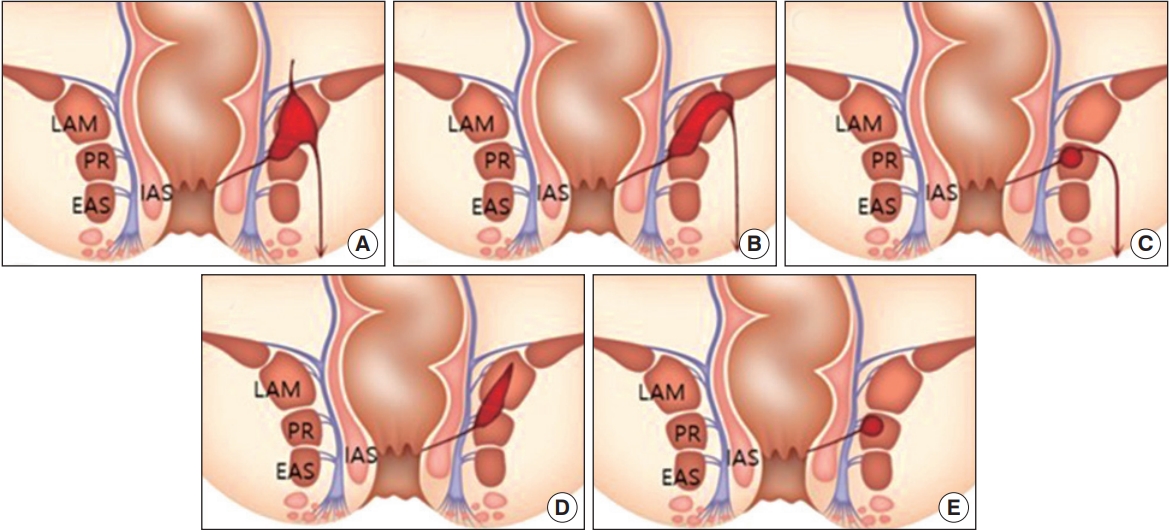
The magnetic resonance imaging findings of patients with puborectalis muscle involvement in suprasphincteric type. Prevalence of type (total 31 tracts) is (A) 1 (3.2%), (B) 5 (16.1%), (C) 14 (45.2%), (D) 3 (9.7%), and (E) 8 (28.8%). LAM, levator ani muscle; PR, puborectalis muscle; EAS, external anal sphincter; IAS, internal anal sphincter.
Surgical method and outcome
We analyzed the surgical outcomes of patients with puborectalis muscle involvement findings on MRI retrospectively. To match the severity of the fistula extrasphincteric type excluded from the Park’s classification, 31 patients with puborectalis muscle involvement in suprasphincteric type were enrolled. The enrolled patients were then divided into 2 groups according to the surgical procedure, the first group underwent the sphincter-saving procedure and the second underwent the sphincter division procedure. For the sphincter-saving procedure, LIFT (ligation of intersphincteric fistula tract) and ALMC (anal duct ligation and muscle closure), the original surgical method of our institution, were used. Also, the sphincter division procedure was performed using the seton procedure. All surgeries were performed by 5 surgeons with over 10 years of experience. Recurrence and complications were diagnosed as clinical symptoms and examinations in the outpatient clinic.
Statistical analysis
Statistical analysis performed using IBM SPSS Statistics ver. 22.0 (IBM Corp., Armonk, NY, USA). Quantitative data were expressed as medians and ranges. Statistical analysis was performed using the paired t-test for paired data. A P-value of < 0.05 was considered statistically significant.
RESULTS
A total of 83 patients (74 males, 9 females; 116 tracts) were included in this study. The tract was missed by MRI scan in 4 patients and wrongly reported in 2 patients. The internal opening was missed in 5 and wrongly reported in 3 patients. The sensitivity and specificity of MRI in diagnosing fistula tracts were 94.8% and 98.2%, respectively. The sensitivity and specificity in identifying internal opening were 93.9% and 97.3%, respectively (Table 1).
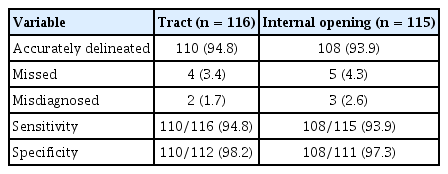
Accuracy of magnetic resonance imaging in complex fistula patients
There were no differences in age, sex, and body mass index (BMI) between the 2 groups. In the previous operation, there were 16 (45.7%) statistically significant fistula operations in the puborectalis involvement group (Table 2). According to the classification SPTF classification, there were 14 patients with simple fistula and 69 patients with complex fistula (Table 2). As per St. James Hospital classification, the features were James type 1 in 6, type 2 in 8, type 3 in 18, type 4 in 15, and type 5 in 36. In addition, according to the Park’s classification, 15 were in intersphincteric type, 30 were in transsphincteric type, 34 were in suprasphincteric type, and 4 were in extrasphincteric type (Table 2). The clinical examination revealed 15 (18.1%) patients were recurrent and 2 (2.4%) were anterior in the female population.
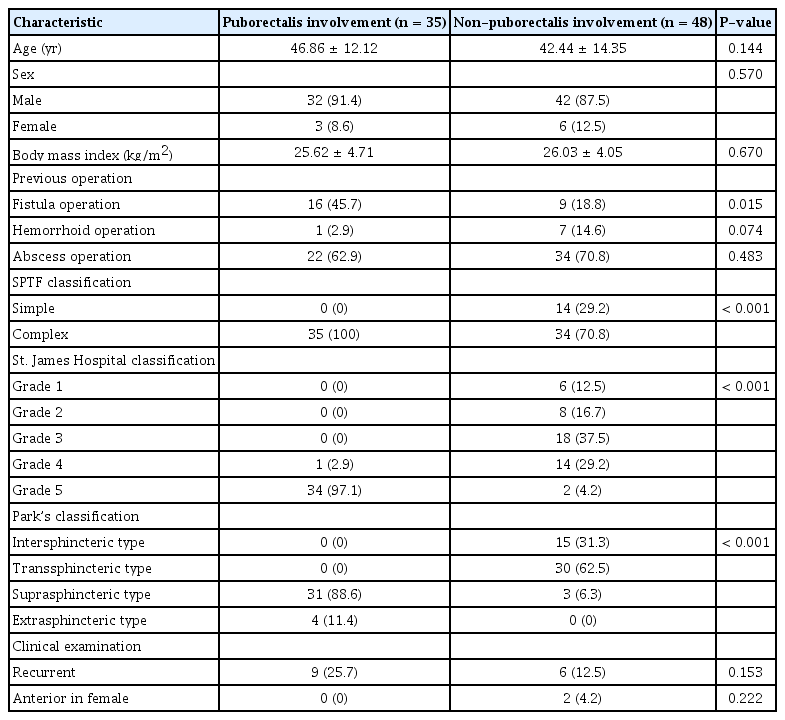
Demographics and clinical characteristics of patients
Table 3 compares the characteristics of fistula between the 35 patients with puborectalis muscle involvement and other patients. In the puborectalis involvement group, the horseshoe tracts were 23 in number and were statistically significantly higher than the non-puborectalis involvement group. Supralevator extension was found in greater numbers in the puborectalis involvement group, while associated abscesses and multiple internal openings were found in greater numbers in the non-puborectalis involvement group, but there was no statistical significance in these findings (Table 3).
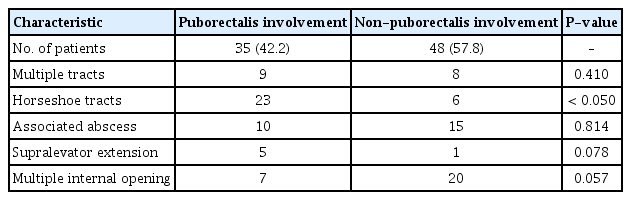
Fistula characteristics of puborectalis muscle involvement on magnetic resonance imaging
Of the 35 patients with puborectalis muscle involvement in the MRI, 31 images of suprasphincteric-type patients on the Park’s classification were classified and shown in Fig. 1. The most common form was where the tract passed through the puborectalis muscle and into the ischioanal space, which was observed in 14 cases. In addition, MRI findings and prevalence of various types of puborectalis muscle involvement are summarized in Fig. 1. The patients mentioned above were divided into 2 groups according to the surgical procedure that was performed. There were 12 sphincter-saving procedures and 19 sphincter division procedures performed (Table 4). When comparing the 2 groups, the BMI was statistically significantly higher in the group that underwent the sphincter division procedure. On the other hand, the length of hospital stay was longer in the sphincter-saving procedure group. Recurrence was seen in 2 patients in the sphincter-saving procedure group, while no case was seen in the sphincter division procedure group. One patient with associated abscess relapsed 4 weeks after the procedure, and another patient showed recurrence 5 weeks after the procedure. There were 2 complications in the sphincter-saving procedure group, but no incontinence was reported. Five complications were found in the sphincter division procedure group, of which 2 reported incontinence.
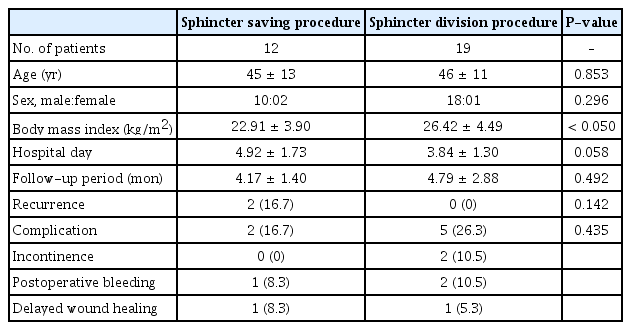
Surgical outcome of suprasphincteric fistula with puborectalis muscle involvement
DISCUSSION
Perianal fistula is a frequent disorder that can cause great difficulties for patients and surgeons. Overall, 5% to 15% of anal fistula tracts have a complicated course, with secondary extensions outside the anal sphincter, often with horseshoe fistulas and ischiorectal or supralevator abscesses [15]. Therefore, to adopt the best surgical strategy and avoid recurrences, it is necessary to obtain precise radiologic information about the location of the fistula tract and the affected pelvic structures [5]. MRI is the most accurate imaging tool to define anal canal anatomy and anal fistulas [16, 17]. Our study measured the diagnostic accuracy of MRI and the importance of puborectalis muscle involvement findings in patients with complex fistulas.
Studies in other countries have been actively conducted. The previous 3 studies from other countries reported the sensitivity and specificity of fistula MRI in transsphincteric type and extra/suprasphincteric type [16, 18, 19]. The sensitivity of MRI for transsphincteric fistulas was reported as 50%, 76%, and 90%, with specificity being reported as 20%, 94%, and 98%. The sensitivity of extra/suprasphincteric fistulas was reported as 50%, 86%, and 94%, while specificity was reported as 90%, 97%, and 98% [16, 18, 19]. Unfortunately, there are very few MRI studies of perianal fistula in South Korea. The reason for lack of study is not only the absence of specialized centers where the surgeons are familiar with anorectal anatomy and the different types of fistula, but there are also problems with medical insurance and high prices. In our study, the sensitivity of MRI was 94.8% and the specificity was 98.2%. Garg et al. [12], affirmed that MRI had remarkably high sensitivity and specificity in predicting the number and location of fistula tracts as well as the position of the internal opening. The sensitivity and specificity in identifying the internal opening were 97.7% and 98.6%, respectively [12]. Similarly, this study also showed a high sensitivity (93.9%) and specificity (97.3%) for finding the location of the internal opening. Through preliminary examination, diseases such as Crohn disease and tuberculosis were excluded, and high MRI accuracy was obtained by using endoanal coils in all patients.
In several studies, radiological evaluation of fistulas with MRI contributed significantly to the surgical management of the disease. Garg et al. [12] have reported that MRI added significant information to the surgical management in 229 patients with additional tract, horseshoe tract, supralevator extension, unsuspected abscess, and multiple internal openings. Using these parameters, they concluded that MRI added significant information to 46.7% of the surgeries. A relatively smaller study of 40 patients by Mullen et al. [20] has shown that MRI positively contributed to the surgical management of the patients. They concluded that the positive contribution of MRI could be as high as 85% if used in selected cases. Our study focused on the clinical significance of puborectalis muscle involvement findings in various parameters of fistula MRI before surgery.
There are 3 clinical implications of puborectalis muscle involvement in patients with complex fistula. First, the puborectalis muscle involvement is valuable as an indicator of complex fistula. In our study, we found that multiple tracts, supralevator extension, and horseshoe tracts were more common in patients with puborectalis muscle involvement findings. Horseshoe tracts were particularly present in relation to the direction of inflammation in the formation of the fistula tract. Shafik [21] had released a new concept that the puborectalis is not part of the levator ani and instead constitute an integral part of the external anal sphincter (EAS) muscle. They created a more complicated division of perianal and perirectal spaces for the dissection of pus and fistula tracts [22, 23] as part of painstaking dissections of the musculofascial septum derived from the terminations and decussations of the longitudinal anal muscle [24]. These findings were at variance with anatomical dissections demonstrating the discrete separation of the deep EAS component from the puborectalis bundle by Fucini et al. [25] and by Fröhlich et al. [26]. These studies have shown puborectalis/EAS separation on CT and MRI with demonstrably separable origins and insertions in plastinated specimens of the adult pelvis [26]. Moreover, the puborectalis muscle is only one horseshoe-shaped muscle in the anorectal area. Thus, the formation of a complex fistula tract and abscess cavity occurs through the puborectalis muscle fascia. Therefore, it is important to approach the complex fistula if MRI shows the involvement of the puborectalis muscle.
Second, the puborectalis muscle involvement findings indicate a variety of clinical features and a customized surgical treatment plan should be established. In 1976, Parks et al. [27] reported all fistulas could be classified into 4 main groups and they suggested that the suprasphincteric fistula tract passes in the intersphincteric plane over the top of the puborectalis. However, in recent studies, puborectalis muscle involvement findings were observed through three-dimensional ultrasonography and MRI [28]. In the present study, 5 types of clinical manifestations were shown in the suprasphincteric fistula with puborectalis muscle involvement. For example, the findings extended to the supralevator and ischioanal spaces as well as a blind pouch was observed in the puborectalis and levator ani muscles. It is necessary to confirm the findings and patterns of puborectalis muscle involvement on MRI before surgery to avoid contact with the unpleasant broad dead space or supralevator extension during surgery.
Third, patients with puborectalis muscle involvement should undergo a sphincter-saving procedure. Studies have reported some degree of fecal incontinence in up to 73% of patients who underwent fistulotomy, according to the risk factors of the patients. These risk factors included preoperative incontinence, recurrent disease, female sex, complex fistula, and previous fistula surgery [29]. There is no clear knowledge concerning the division of any part of the anal canal during the treatment of perianal fistula. However, it is clear that puborectalis muscle contraction is the independent variable with the strongest correlation to the clinical severity of incontinence [11]. In the present study, there were 2 patients with incontinence complications; both showed these complications after the sphincter division procedure. Both patients were young men, and symptoms of incontinence were not severe and could be controlled by conservative treatment. The anterior EAS is shorter in females and the percentage of compromised muscles is high [30]. However, in our study, female incontinence complications were not seen due to the low participation of female patients. Studies in the literature are contradictory concerning the amount of sphincter muscle that can be safely divided in anal fistulas, with some reporting that the division of less than 30% of the EAS carries a minimal risk of postoperative fecal incontinence [31]. Conversely, Garcés-Albir et al. [32] reported that the division of the lower 66% of the EAS was associated with excellent rates of continence and healing in patients who lacked risk factors before surgery. Although the results are limited due to the small sample size, the surgical outcome of this study suggested that patients with puborectalis muscle involvement seen in an MRI should undergo a sphincter-saving procedure.
Our study does have some limitations. Firstly, all interpretations of the MRI scans were by a single radiologist, and therefore, interobserver variability could not be determined. Secondly, the operating surgeon was not blinded to MRI findings. Both of these factors were the sources of potential bias in this study. Thirdly, the decision of surgical procedure was determined by the operator’s preference. BMI was significantly higher in sphincter division procedure because high BMI interfered with the surgical field of view. This was the source of selection bias in this study. In the future, a prospective study of large volumes will examine the relationship between puborectalis muscle involvement and surgical procedures.
To conclude, fistula MRI is a highly accurate examination for evaluating complex fistulas, and the puborectalis muscle involvement findings are very important for diagnosis and treatment planning for complex fistulas.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.