INTRODUCTION
Diverticular disease is a common disorder occurring in elderly people, and its incidence is increasing. No more than 20% of the patients with colonic diverticulum have symptoms, and of those who have symptoms, 25% experience complications such as abscess, perforation, stricture or fistula. Adult intussusception represents 5% of all cases of intussusception and accounts for only 1-5% of intestinal obstructions in adults [1]. Almost 90% of intussusceptions in adult are secondary to a carcinoma, polyp, stricture or benign neoplasm, including a colonic diverticulum [2]. A giant colonic diverticulum (GCD) is a rare entity of disease and is defined as a diverticulum greater than 4 cm in size [3]. More than 90% are antimesenteric and arise from the sigmoid colon [4]. Several GCDs have been reported, almost all of which developed at old age and in the sigmoid colon [5, 6]. We report a case of a GCD, which was removed by using a laparoscopic colectomy. To our knowledge, this is the first case of an ascending GCD in a young adult that suggests a congenital origin in pathogenesis and presented with intussusceptions.
CASE REPORT
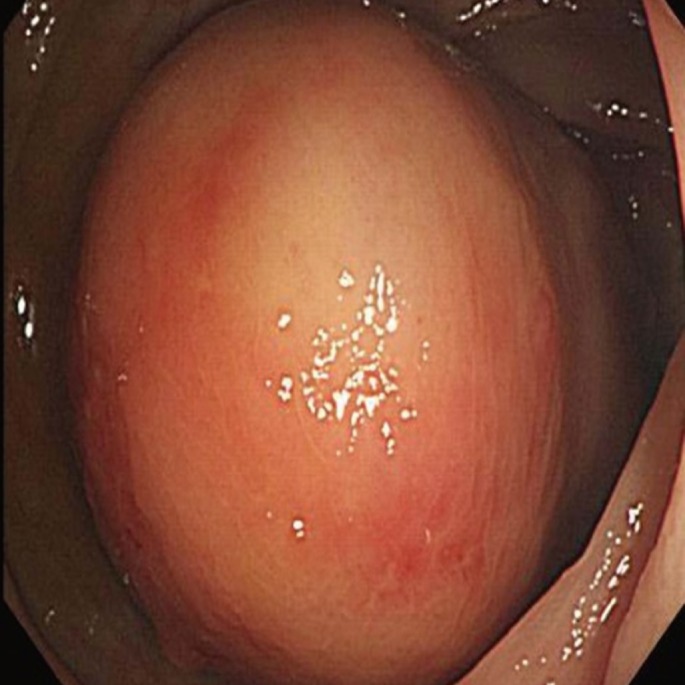
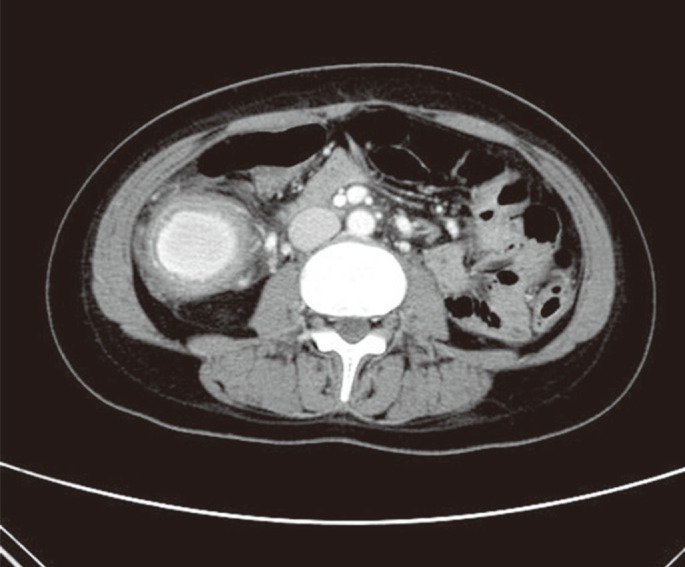
A 30-year-old female was transferred to Chosun University Hospital with a 1-month history of left lower quadrant pain. The laboratory examination at admission was unremarkable. Physical examination revealed left lower quadrant tenderness with a palpable abdominal mass. Plain abdomen X-ray presented a gas-filled cavity in the middle right abdomen. The computed tomography scan from an outside hospital showed a target sign suggesting intussusception in the mid to lower colon on the left side (Fig. 1). The intussusception was soon resolved spontaneously without any procedure. To evaluate the lesion, we performed a colonoscopic examination, which revealed a huge submucosal tumor (SMT)-like lesion in the ascending colon (Fig. 2). The abdominal computed tomographic scan was checked again for further assessment of the SMT-like lesion and showed 4.2-cm-sized encapsulated fluid of high density with a thick wall on the right side of abdomen (Fig. 3).
A laparoscopic right hemicolectomy was performed because of uncertainty of the diagnosis and for a one-stage treatment. On the operation findings, the lesion which was 5 cm ├Ś 5 cm in size was located in the mid portion of the ascending colon and extended to the hepatic flexure. Also, multiple enlarged lymph nodes were found around the ileocolic and the middle colic vessel and were removed by using an en bloc resection. Gross finding of the removed specimens showed a large diverticulum on the ascending colon (Fig. 4A). Histologic examination of the diverticulum showed the full thickness of the bowel wall from the mucosa to the serosa (Fig. 4B). The patient made a quick recovery and was discharged 7 days after surgery without any complication.
DISCUSSION
Colonic diverticular disease is a common condition and rarely presents as a singular giant diverticulum. A GCD, which is greater than 4 cm in size, is an uncommon manifestation of colonic diverticular disease and mainly occurs solitarily in the sigmoid colon [5, 7]. The pathogenesis of a GCD is not well established. Possible theory supports a ball-valve mechanism through a tiny communicating neck, which causes air entrapment so that the diverticulum increases in size. Another theory postulates that the formation and the enlargement of a GCD is secondary to gas-forming organisms [8]. There are different types of GCDs. Steenvoorde et al. [9] described a histological classification of three distinct subtypes of GCDs. Type I is a pseudo-diverticulum containing remnants of the muscularis mucosa and the muscularis propria, and this type of diverticulum is found in colonic diverticular disease. Type II is an inflammatory GCD resulting from a local perforation of the mucosa with a persistent abscess cavity retaining contact with the colonic lumen, and the type III is a true diverticulum containing all layers of a normal bowel.
The clinical presentation of a GCD can be asymptomatic, but patients present most commonly with abdominal pain, constipation, or a palpable, nontender, abdominal mass [9, 10]. A plain abdominal X-ray is used as the first line for diagnosis of a GCD. It is the simplest and most readily available tool and can reveal a large air-filled structure with or without fluid levels. A barium enema can demonstrate communication with the large bowel lumen in the majority of cases [11], but fails in approximately one-third of reported cases [7, 9]. The differential diagnosis for a GCD includes sigmoid or caecal volvulus, a duplication cyst or giant Meckel diverticulum, and pneumatosis cystoides intestinalis [3].
A plain supine abdominal X-ray is the simplest and most readily available diagnostic tool and should be used as the first line in suspected cases because it can reveal a large air-filled structure (balloon-like appearance) with or without fluid levels. Computed tomography shows a smooth, thick-walled, air-filled structure intimately associated with the colon [8]. Colonoscopic evaluation is difficult in diagnosing a GCD. The ostium between the diverticulum and the colon is frequently too small to be detected [7-9]. GCD cases that have spontaneously resolved with conservative treatment have been reported; nevertheless, the gold standard of management of a GCD is a surgical resection and a primary anastomosis to exclude an underlying malignancy because adenocarcinomas arising from GCDs have been reported previously [9].
In the era of minimal invasive surgery, a laparoscopic colonic resection including the lesion and a primary anastomosis may be feasible in most patients. Laparoscopic surgery has advantages of fast recovery, reduced hospital stay, less pain and better cosmesis [11, 12]. Our case has some differences compared with previous cases. The lesion in our patient occurred in the ascending colon, not the sigmoid colon even though. The histological classification of our case was a true diverticulum, and the origin of diverticulum in our case might have been congenital because the patient was a young adult, unlike most GCD cases where the patients are much older. Our patient was treated with a laparoscopic right hemicolectomy, and there have been no symptoms or signs of recurrence since then (2 years).