INTRODUCTION
Nowadays, diverticulitis is one of the most common benign conditions in industrialized countries, and its prevalence has been increasing over the last century. The latest studies show that the prevalence of the disease increases with age. Indeed, while diverticular disease affects 5% to 25% of adults up to an age of 50 years, this proportion rises to 60% above 80 years of age [1]. The disease is usually asymptomatic, although approximately 10% to 25% of the subjects diagnosed with diverticular disease will develop an episode of acute diverticulitis [1, 2].
While common, this pathology is still widely discussed. Indeed, the best management of a first episode of uncomplicated diverticulitis remains somewhat controversial as is demonstrated by the numerous recommendations from different societies [1, 3]. However, the majority of patients presenting with simple diverticulitis will still be conservatively and successfully managed with antibiotics and dietary modification [1, 4]. The rationale being that a majority of patients treated for a first episode of acute inflammation will eventually recover and have no further problem [1, 5]. A recent Swedish multicentric randomized trial has shown that antibiotic treatment for acute uncomplicated diverticulitis neither accelerates recovery nor prevents complications or recurrence, leading to a proposal to reserve antibiotics for the treatment of complicated diverticulitis [6]. In addition, several studies have shown that ambulatory care can be provided to selected patients with uncomplicated diverticulitis [1, 4, 7]. As the type and length of antibiotic therapy is not standardized, no consensus is agreed in uncomplicated diverticulitis treatment.
The aim of this study was to review all patients treated at our facility for a first episode of uncomplicated diverticulitis according to the length of antibiotic treatment. Recurrence risk and treatment failure were evaluated by comparing the results from shortversus long-term intravenous (IV) antibiotics therapy.
METHODS
From January 2007 to February 2012, data on all the patients presenting at our facility with a first episode of uncomplicated diverticulitis, as confirmed by computed tomography (CT) [8, 9], and requiring hospitalization were prospectively collected into a protected database. A prospective follow-up was conducted by a specialized research nurse (B.K.). An informed consent was required and obtained from all patients. This study was approved by our local ethical committee and registered in Clinicaltrials.gov with the identifier number NCT01015378. We also performed an auxiliary analysis for the patients who were included in our database [5].
Diverticulitis was diagnosed based upon physical examination and laboratory tests revealing an inflammatory syndrome and was confirmed by using an abdominal CT scan [5]. The disease severity classification chosen for this study was the modified Hinchey classification [3, 10, 11]. Exclusion criteria were complicated diverticulitis (Hinchey-Ib class and above), under 18 years of age, chronic inflammatory bowel disease or a tumor, and refusal to consent.
At our institution, we usually prefer an initial IV therapy for an inpatient management. All patients received an IV antibiotic treatment of ceftriaxone (2,000 mg/day) and metronidazole (1,500 mg/day) except when contraindicated. For the purpose of this study, the patients were divided into 2 groups according to the length of IV treatment: the first group received an IV antibiotic treatment for 5 days or less; the second received an IV treatment for 6 days, possibly up to 14 days. There was no randomization. The choice of the length of the treatment was decided on a case-by-case basis by the surgeon in charge of the patient. Of note, the patients who received a 5-day IV treatment were also given an additional 5-day course of oral antibiotics (1,000-mg/day ciprofloxacine and 1,500-mg/day metronidazole) to complete the treatment. As soon as a clinically successful treatment had been achieved (absence of fever, absence of peritonitis or abdominal complaints, and diminution of inflammatory markers), the patient was discharged.
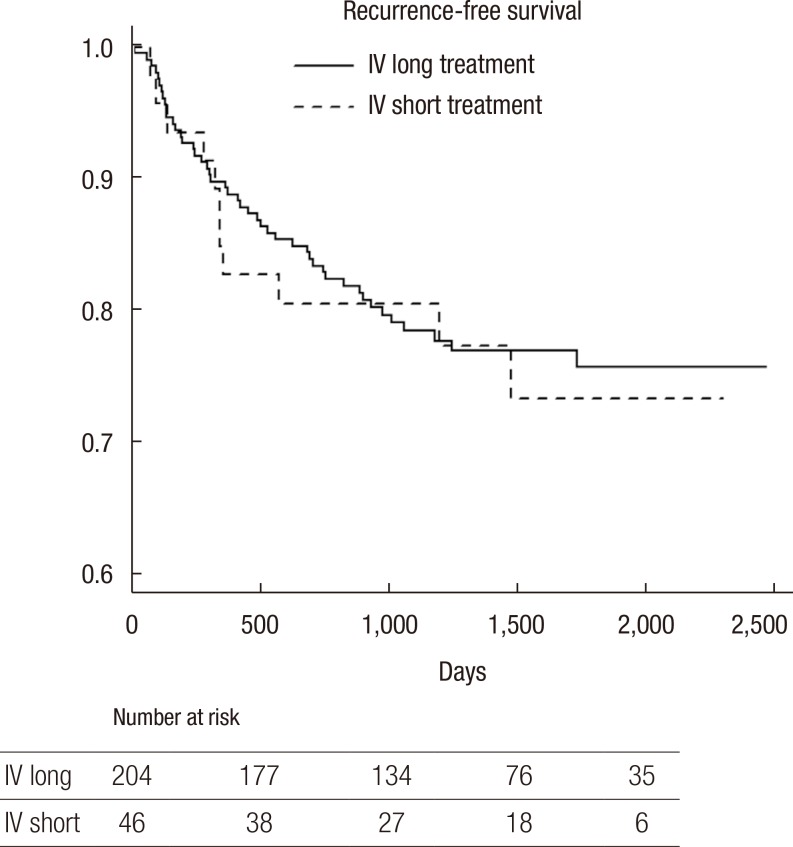
The primary outcome was the recurrence-free survival time. Only patients with a follow-up of at least 12 months were included in this analysis. A recurrence was defined as a readmission at 12 weeks or more after the previous episode and the complete resolution of inflammation parameters. Diagnosis was confirmed by using a CT scan in all cases. Any recurrences within 12 weeks of the first episode were considered as an ongoing diverticulitis. Any early readmissions were analyzed as well in order to rule out failure of the treatment.
Data are reported as means ┬▒ standard deviations or as medians and ranges for continuous parameters. Categorical variables are reported as percentages. Comparisons of clinical and demographical parameters between short- and long-term IV treatments were assessed using the chi-square test for discrete variables and the Student t-test for continuous variables. The recurrence free survival functions of the two treatment groups were estimated using the Kaplan-Meier method and were compared using a log-rank test. Statistical significance was assessed at the 0.05 level for all analyses. All analyses were performed with R ver. 2.15.2 (R Foundation for Statistical Computing, Vienna, Austria)
RESULTS
Two hundred eighty-two patients were followed after a first episode of acute uncomplicated diverticulitis (Hinchey Ia) with at least a one-year follow-up. Two hundred sixty patients were initially treated with IV ceftriaxone and metronidazole (90.9%); 3 patients were treated with IV ciprofloxacine and metronidazole; 6 with piperacilline/tazobactam; and 12 with imipenem/cilastatin. One patient was initially treated with IV ceftriaxone and metronidazole, which was switched to imipenem/cilastatin because after three days of hospitalization, the patient was symptomatic with an increasing white blood cell (WBC) and C-reactive protein (CRP).
The mean follow-up was 50 ┬▒ 17 months (range, 19-89 months). Follow-up was lost in eleven patients. Follow-up was completed for 271 patients-136 women and 135 men-with a median age of 56 years (range, 24-85 years). Only patients treated with IV ceftriaxone and metronidazole were included in the analysis (n = 256 patients), of whom 46 patients (18%) received an IV antibiotic treatment for a maximum total duration of 5 days. Two hundred ten patients (82%) received a long IV antibiotics treatment (6 to 10 days).
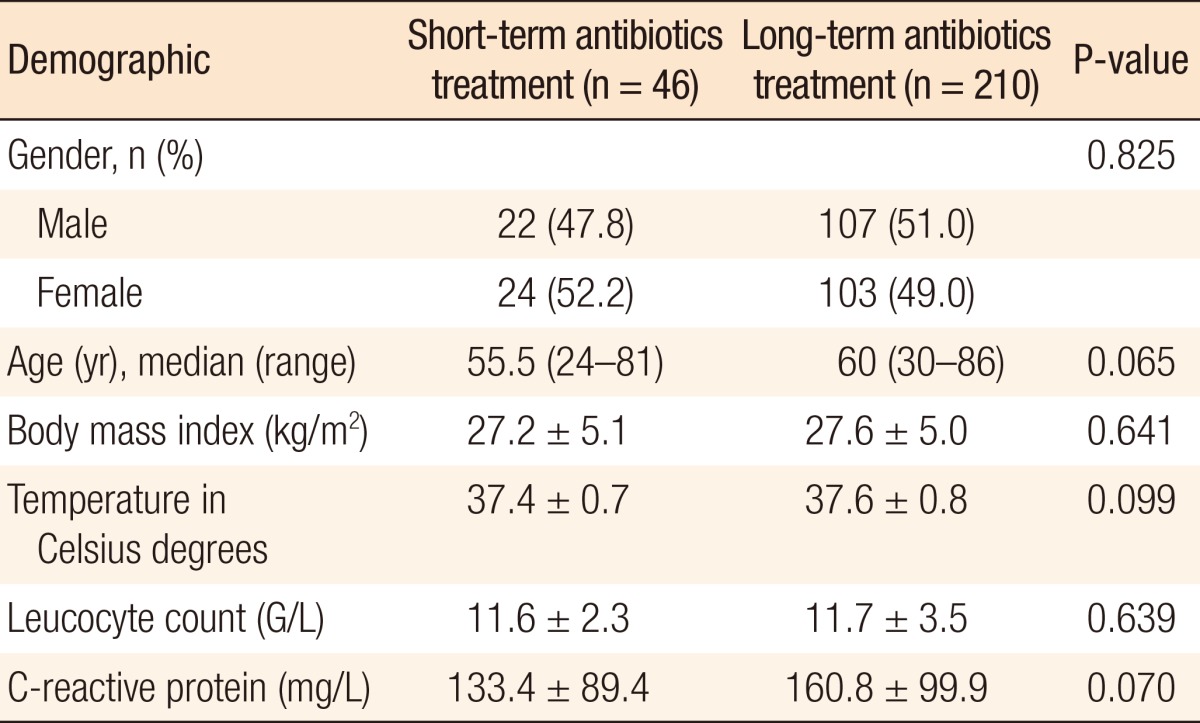
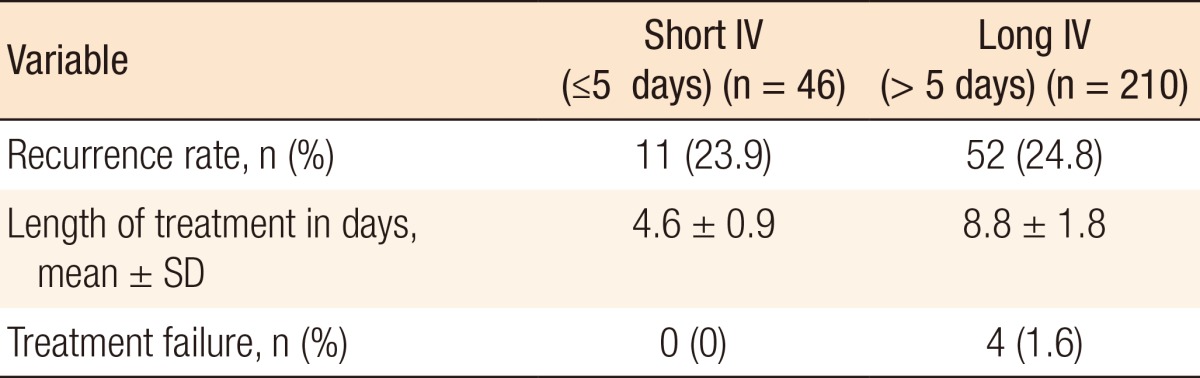
As shown in Table 1, no differences in the clinical and the demographic characteristics (gender, body mass index, temperature, CRP level and WBC) were measured during the first hospitalization, and no mortalities occurred. For the 46 patients in the short IV treatment group, the mean length of treatment was 4.7 days. Eleven patients (23.9%) experienced recurrence for a total of 185 person-years, resulting in a 100-person-year incidence rate of recurrence of 5.95. Of the patients with recurrence, no patients underwent an emergent surgical procedure. On the other hand, four underwent an elective sigmoidectomy.
Concerning the 210 patients in the long IV treatment group, 52 episodes of recurrence (24.8%) were observed for a total of 882 person-years, resulting in a 100-person-year incidence rate of recurrence of 5.89. The mean duration of treatment was 8.7 days (Table 2). Of the patients with recurrence, five underwent an emergent surgical procedure: three Hartmann operations and two laparoscopic drainages. Moreover, 41 patients underwent an elective sigmoidectomy.
Fig. 1 shows the recurrence-free survival for short IV treatment versus long IV treatment. No statistically significant difference in the recurrence-free survivals between the two treatments were observed, as was confirmed by the log-rank test (P = 0.772), in patients with uncomplicated diverticulitis. Treatment failure was observed in only four patients, who were readmitted for pain and fever (1.6%). All of them were in the long-course treatment group (Table 2). The CT scan showed for all patients a phlegmonous diverticulitis (Hinchey Ia).
DISCUSSION
Recent international guidelines for the treatment of uncomplicated acute diverticulitis suggested a nonoperative treatment with dietary modification and the administration of oral or IV antibiotics [1, 3]. Nevertheless, the management of a first episode of uncomplicated acute diverticulitis remains somewhat controversial [3]. Among potential problems, the possibility of antibiotic resistance among bowel bacteria has been raised [12]; thus, the real need for antibiotics has been questioned [13]. A recent Swedish multicentric randomized clinical trial showed that antibiotics do not prevent surgical complications or recurrences and should, thus, be reserved for patients with complicated diverticulitis. In the Swedish study, the patients were randomized according to treatment with or without antibiotics; complications such as perforation and abscess formation were found in six patients (1.9%) who received no antibiotics and in three (1.0%) who were treated with antibiotics (P = 0.302). The incidences of recurrent diverticulitis necessitating re-admission to the hospital at the 1-year follow-up were similar in the two groups (16%, P = 0.881) [6]. Similar results were reported by de Korte et al. [13] in a retrospective case-controlled study. Overall, there is little evidence that routine administration of antibiotics influences the course of uncomplicated diverticulitis, even though almost every international guideline advices their use [3].
We present herein a large prospective study evaluating the natural history of uncomplicated diverticulitis [5]. After an average follow-up of 50 months, the risk of recurrence did not appear to be different after a short- or a long-term IV antibiotic treatment. Indeed, in our cohort, the recurrence rate, 24%, was similar between the two groups. More interesting, the risk of early readmission was similar between the two groups, as well. Reducing the length of IV treatment might allow us to diminish the length of stay, which is clearly cost effective for the patient, the institution and society. Our results show that the treatment of diverticulitis for inpatients is possible with a shorter duration of IV antibiotic treatment. Similar findings were reported by other centers where short-duration IV treatments were found not to have modified the recurrence rate in patients with uncomplicated diverticulitis [14, 15].
Schug-Pass et al. [14] showed that short-term ertapenem therapy (4 days) was as effective as longer therapy (7 days) for the treatment of uncomplicated diverticulitis. Interestingly, 13.8% of the patients, a minority, dropped out during the course of the study because of persistent symptoms. Furthermore, a treatment as short as possible is strongly recommended by the Surgical Infection Society [16].
This study has some limitations that deserve a word of caution. First, by its nonrandomization nature, a bias of selection might exist. Because the choice of the length of treatment was decided by the surgeon in charge, we admit that potentially good patients could have received the short-term treatment; however, according to the CT scan classification, no differences existed. On the other hand, more fragile or at risk patients might have been allocated to the long-term treatment, which might not have been seen when comparing the patients' characteristics because both populations were similar in terms of demographics and initial severity of disease; nevertheless a trend was seen (higher CRP in the long-duration IV treatment group).
The majority of patients presenting with a first episode of uncomplicated diverticulitis are hospitalized in our institution. Indeed, our policy of ambulatory care for acute diverticulitis is relatively conservative. The decision to hospitalize a patient for uncomplicated diverticulitis depends, of course, on the patient's clinical status [14, 15]. While we are a referral center, we admit all patients, especially those with many comorbidities. A certain proportion of patients with milder disease are treated in ambulatory facilities by general practitioners (often without a CT scan), and those were not included. These need to be mentioned as biases of selection because the good patients would never be admitted to our institution, but would have uncertainties in their diagnoses (only 60% of patients with left pain actually have acute diverticu-litis). On the other hand, hospitalizing all patients would be inter-esting in this situation because that would allow us to determine more accurately the true incidence and recurrence rates of diver-ticulitis [5].
In addition, the short-term group did receive another five days of oral antibiotics, which could render the interpretation of the data difficult. Whether the similar recurrence rates between the two groups should be considered as a success of oral antibiotics is not clear. Indeed, oral antibiotics seem to be as effective as IV antibiotics [17].
Overall, this study allowed us to standardize our management for acute documented Hinchey Ia diverticulitis with a shorter IV antibiotic (ceftriaxone and metronidazole) treatment. This strategy has been proven safe by some other group [15]. Of course, the clinical and biological evolution remains the main parameter to consider. The management of acute diverticulitis must be tailored to the patient's need. This study allows us to recommend a shorter antibiotic treatment, aiming to reduce the length of hospital stay for patients in good general condition. We face an increased admissions rate for this indication, as reported by Etzioni et al. [18] for the United States.
We must find acceptable solutions without impairing the management of our patients. Shorter antibiotic treatment could play a key role and was safe for the patients in our case-controlled series. The present study results provide strong arguments regarding the safety of a short IV antibiotic treatment. The short IV treatment does not modify the recurrence rate in patients with uncomplicated diverticulitis; the risks of treatment failure were similar as well.