INTRODUCTION
Among several lipomatous tumor variants, a myolipoma is a very rare benign lesion composed of mature adipocyte and benign smooth muscle fibers. Although the pathogenesis of a myolipoma remains unclear, there are two main theories that explain the mechanism: namely, adipose metaplasia and a multipotential Müllerian cell origin [1]. A myolipoma is mostly found incidentally in the deep soft tissue of the abdomen or retroperitoneum. However, there have been very few cases in which the tumor has affected other anatomical sites. Because all the surgically-treated myolipomas that have been reported have been benign regardless of their location, normally a complete surgical excision is performed for the treatment of these lesions. To date, no case of an anal myolipoma has been reported in the English literature. In this report, we present the first case of a surgically-resected myolipoma on the anal margin.
CASE REPORT
A 30-year-old female presented with a progressively growing perianal mass. The mass had been slowly increasing in size for 17 years. Physical examination showed a 6 × 4 × 4 cm3, firm, ovoid mass with a wide pedicle extending to the anal margin at 2 to 10 o'clock (Fig. 1). The mass was apart from the vagina and had a somewhat firm and cord-like lesion within a pedicle. She also had grade II to III internal hemorrhoids at 3 and 7 o'clock. Nothing remarkable was noted in the laboratory work-ups, including complete blood cell count, blood chemistry, urinalysis, and plain chest radiograph.
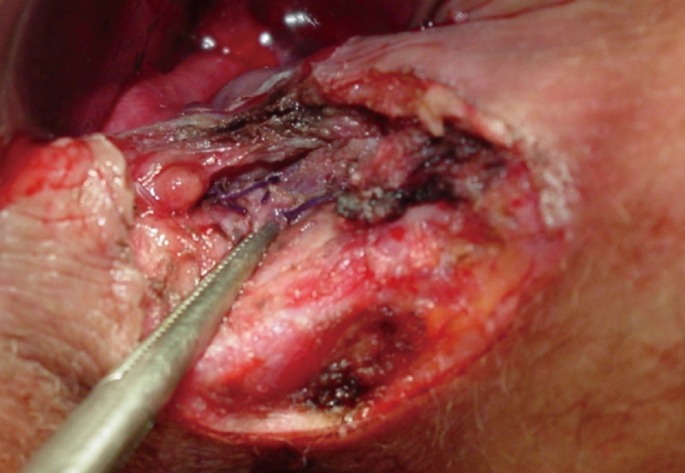
A wide surgical excision was performed. A cord-like lesion arising in the intersphincteric groove was the root of vessels and was treated by suture ligation (Fig. 2). Concurrently, her hemorrhoids were treated by ligation and excision.
Macroscopically, the tumor was well-encapsulated, and the consistency was a little firm.
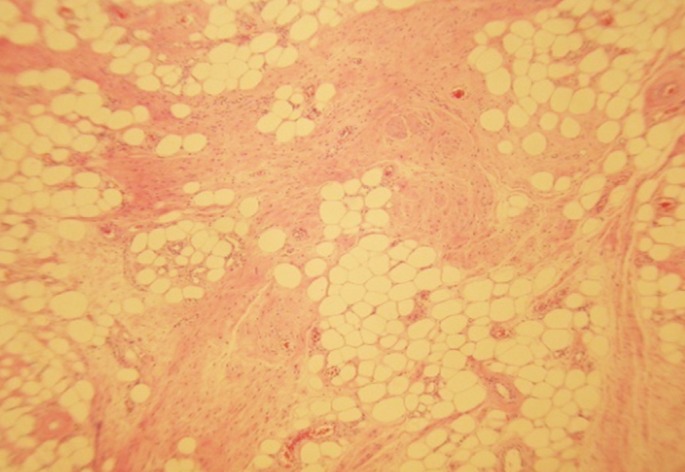
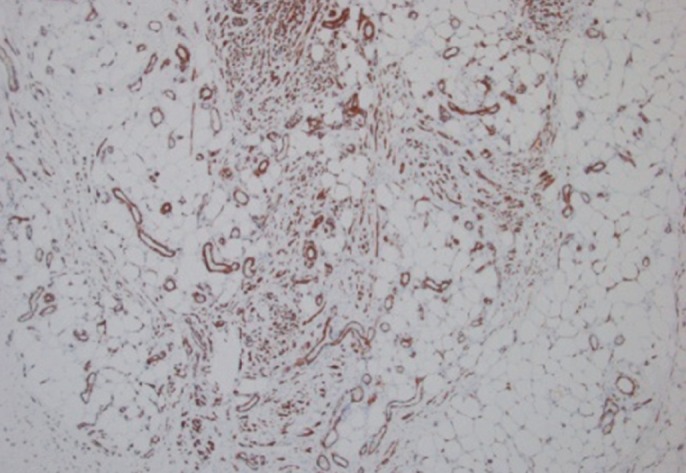
The cut surface contained gray-white or yellowish areas (Fig. 3). Microscopically, the tumor was composed of mature adipose tissue and smooth muscle fibers. They were intermingled with each other irregularly. Abundant dilated and thin-walled blood vessels were observed, but neither mitosis nor cellular atypia was shown (Fig. 4). Immunohistochemically, the smooth muscle fibers and blood vessel walls were positive for smooth muscle actin, but negative for CD34, c-kit and HMG-45 (Fig. 5).
The patient recovered without any postoperative complications. We carried out follow-ups regularly for 6 months, and she showed no evidence of recurrence.
DISCUSSION
In the literature, benign tumors of the anal margin may range from innocuous in situ Bowen's disease to clinically aggressive verrucous lesions [2]. However, no obvious statistical data for benign tumors arising from the anal margin are available. According to the World Health Organization's classification of soft tissue tumors in 2002, benign lipomatous lesions are classified into nine categories: lipoma, lipomatosis, lipomatosis of nerves, lipoblastoma/lipoblastomatosis, angiolipoma, myolipoma, chondroid lipoma, spindle cell/pleomorphic lipoma, and hibernoma [3]. Among these lipomatous lesions, a myolipoma of soft tissue is a very rare benign lipomatous lesion [4].
In 1991, the first nine cases of a soft tissue myolipoma were described by Meis and Enzinger [5]. They reported nine cases of a previously undescribed benign soft tissue tumor: one in the subcutaneous adipose tissue, one in the rectus sheath of the anterior abdominal wall, two within the abdominal cavity attached to the abdominal wall, two in the inguinal region, and three in the retroperitoneum [5]. It has also been reported in various anatomical sites, including the spinal cord, orbit, round ligament, and breast [6-9]. Myolipoms occur most frequently in adults in their 5th and 6th decades of life, with a female predilection (2:1 ratio) [4]. Grossly, these tumors are usually completely, or at least partially, encapsulated and have a yellow to white appearance. A histological analysis demonstrates a variable admixture of smooth muscle and mature adult adipose tissue [4]. The smooth muscle component often predominates, with a typical ratio of 2:1 (muscle to fat) [10].
In our case, microscopic findings closely mimicked those of an angiomyolipoma (AML) because of abundant vessels. However, this tumor was immunohistochemically negative for HMB-45 staining and contained no medium-sized arteries distinctive of an AML. AML is also a rare soft tissue tumor and probably a hamartomatous process, which is mostly found in the kidneys [11]. It is usually associated with tuberous sclerosis or is sporadic [12]. Furthermore, extrarenal AMLs are very rare tumors that have been reported in various organs, including the liver (second most common site), colon and skin [11, 13, 14]. Although the majority of AML cases follow a benign course, malignant transformation of an AML has also been reported [15]. In previously reported cases of a myolipoma, neither postoperative recurrence nor metastasis has been noted, and both the histological appearance and the clinical course suggest that it has a benign nature. Here, we conducted a careful follow-up survey to identify any long-term complications.
In conclusion, we report a case of a myolipoma arising from the anus. Thus, consideration of a soft tissue myolipoma in the differential diagnosis of fat-containing lesions of the anus is important if an accurate diagnosis is to be made.