INTRODUCTION
Neutrophil-to-lymphocyte ratio (NLR) has been implicated with adverse oncological outcomes among colorectal cancer (CRC) patients, associated with worse overall survival (OS) and recurrence-free survival (RFS) [1]. It has also been often used as a surrogate marker of systemic inflammatory response.
The link between individual inflammatory response and cancer development has been first suggested by Virchow in 1881 [2], and studies in recent years have investigated the utility of inflammatory biomarkers: plasma C-reactive protein, albumin, total white blood cell (TWBC) count and derived differential ratios such as NLR [3], and their prognostic value on various malignancies [4-7] including CRC [8].
CRC patients of 10% to 20% first present with bowel obstruction [9, 10]. While upfront surgery was often indicated, since the introduction of endoscopic self-expandable metallic stent (SEMS) placement for CRC in 1991 [11], the use of SEMS as a bridge to elective curative surgery has been gaining acceptance and increasingly adopted for patients presenting with bowel obstruction [12].
Among these patients, the prognostic accuracy of NLR may be influenced by the presence of tumor obstruction [13], obstructive ileocolitis [14], and resultant dehydration. In addition, endoscopic stenting can induce a local desmoplastic reaction and trigger an inflammatory response [10, 15]. These factors may further confound TWBC and NLR values. Therefore, it remains unclear whether NLR is a useful prognosticating tool in patients with obstructing CRCs who have undergone SEMS placement prior to curative surgery.
This study evaluates the prognostic value of NLR among patients with obstructing CRC who were successfully stented as a bridge to curative surgery.
METHODS
Between January 2007 and December 2016, 62 patients presented with obstructing CRC at Singapore General Hospital, and underwent endoscopic placement of SEMS as a bridge to curative surgery. Large bowel obstruction was confirmed clinically and radiologically. All patients underwent a computed tomography (CT) scan of the abdomen and pelvis at initial presentation. Full staging CT scans were done either at diagnosis or within 30 days of presentation. There was no evidence of distant metastasis within this cohort of patients. All patients received antibiotics upon admission, before the stenting procedure was commenced. One technical failure and one stent perforation were encountered, with both patients requiring emergency operation on the same day. Three other patients had minimal bowel decompression after endoscopic placement of SEMS and were operated within 48 hours. A total of 57 patients who had successful bowel decompression after SEMS deployment, followed by elective curative surgery, were included in this study. The study was approved by the Institutional Review Board of Singapore General Hospital (No. 2017/2481).
Clinical, histopathological, survival, and oncological data were retrospectively reviewed from a prospectively maintained database. Clinical data including patient demographics, biochemical results, and radiological findings were collected from a computerized database (Sunrise Clinical Manager ver. 5.8, Eclipsys Corp., Atlanta, GA, USA). Endoscopic and surgical data were collected from another server (OTM 10, IBM Corp., Armonk, NY, USA).
NLR was calculated from the differential WBC counts obtained at presentation, and at least 4 days after successful SEMS deployment, before elective surgery. Apical lymph node was defined as the lymph node at the origin of the inferior mesenteric artery. Where possible, all patients were considered for adjuvant chemotherapy in the form of capecitabine and oxaliplatin under the guidance of the oncologist. The postoperative surveillance protocol has been described in an earlier study [16]. RFS was defined as the time period from surgery to the date of detection of radiological and/or pathological CRC recurrence. OS was calculated from the time of surgery to the date of death or latest date of follow-up.
Patient demographics and tumor characteristics were presented in median (interquartile range) for continuous variables and count (percentage) for categorical variables. The OS of 3- and 5-year and the 95% confidence interval (CI) were presented. Differences in clinicopathological features between the 2 groups were analyzed using the chi-square or Fisher exact test for categorical variables where appropriate, and the Student t-test for continuous variables. Each variable was analyzed by univariate Cox regression model for OS and RFS, respectively. Those variables with P-value of < 0.10 and clinically relevant variables were entered into multivariable Cox regression model. The variables were selected into the respective final model using stepwise approach with significant entry level at 0.10 and significant exit level at 0.05. The results of Cox regression model were presented in estimated hazard ratio (HR) with 95% CI and Wald test P-value. Both OS and RFS curves were estimated using Kaplan-Meier method and plotted up to 72 months.
Optimal cutoff to dichotomize NLR was obtained by maximizing log-rank test statistic with recursive partitioning of Kaplan-Meier RFS and OS curves. Cutoff was initiated from 2.0 with 0.5 increment for subsequent test. Optimal cutoff was determined once 2 greater consecutive P-values of log-rank test were obtained. For NLR values calculated at presentation before stent deployment, the optimal cutoff value was NLR ≥ 5. As for NLR values obtained after stent deployment before elective curative surgery, the optimal cutoff for high NLR was ≥ 4 (Supplementary Tables 1, 2; Supplementary Fig. 1). Statistical analysis was done using SAS ver. 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Fifty-seven patients with obstructing CRC were decompressed successfully via SEMS placement, followed by elective curative resection of the primary tumor. There were 23 patients in the high NLR (H-NLR) group with preoperative NLR of ≥ 4 and 34 patients in the low NLR (L-NLR) group with preoperative NLR of < 4. The clinical and oncological details of the patients are summarized in Table 1. The median duration from stenting to surgery of 10.5 days (range, 6 to 23) in the H-NLR group did not differ significantly from the 10 days (range, 5 to 18) in the L-NLR group (P = 0.913).
Comparison of baseline characteristics between the 2 groups showed no significant differences in demographics such as age and gender. A majority of the patients were surgically fit (American Society of Anesthesiologists physical status classification I to II) (n = 50). In the H-NLR group, there were a greater proportion of patients with elevated preoperative carcinoembryonic antigen (CEA) 5.3 μg/L (69.6% vs. 44.1%, P = 0.058), and more patients had T4 tumors (30.4% vs. 14.7%, P = 0.153), although these were not statistically significant.
The patients in the H-NLR group were significantly associated with higher rates of apical lymph node involvement, and lymphovascular invasion on histology. The surgical resection margins were clear macroscopically and microscopically in all cases within this study, with a mean of 21.7 lymph nodes harvested. While all patients had primary anastomosis after tumor resection, the formation of a temporary diverting stoma was undertaken in 4 patients in the H-NLR group, at the intraoperative discretion of the individual surgeon. Although there were no differences between the 2 groups in terms of the overall rate of postoperative morbidity, 3 patients in the H-NLR group had major complications, including 2 with anastomotic dehiscence and 1 patient who demised postoperatively from septic complications secondary to pneumonia. There was no difference in the proportion of patients who received adjuvant chemotherapy. There was a higher proportion of H-NLR patients who developed metachronous distant metastases (56.5% vs. 32.4%, P = 0.070), with the P-value approaching but not reaching statistical significance.
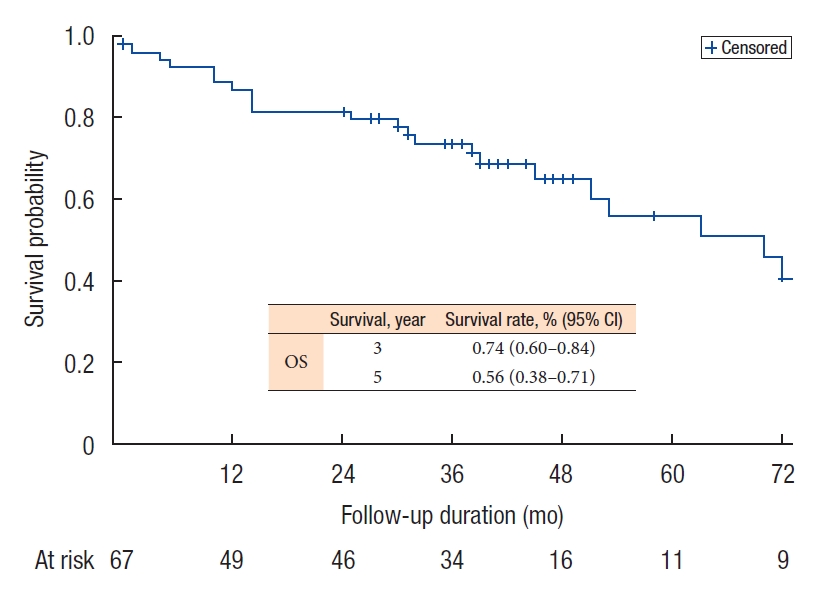
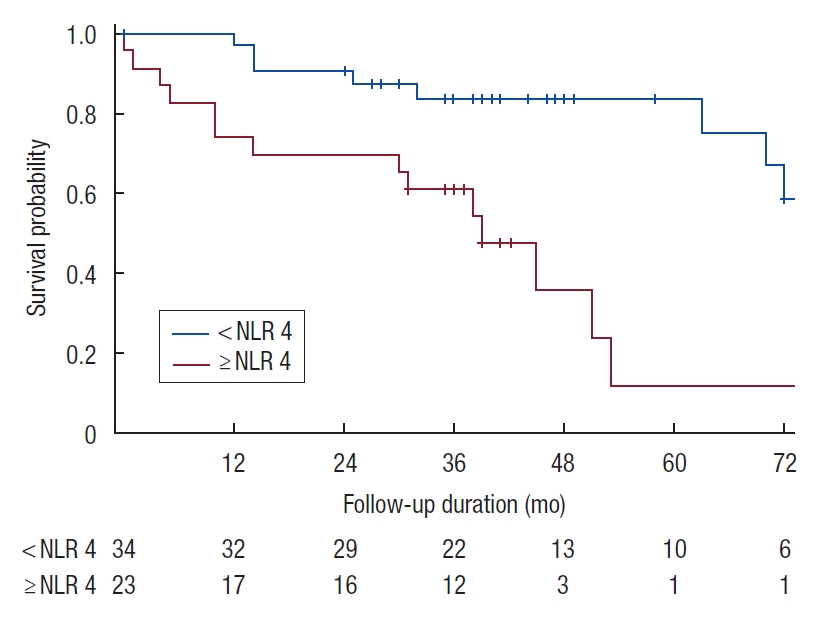
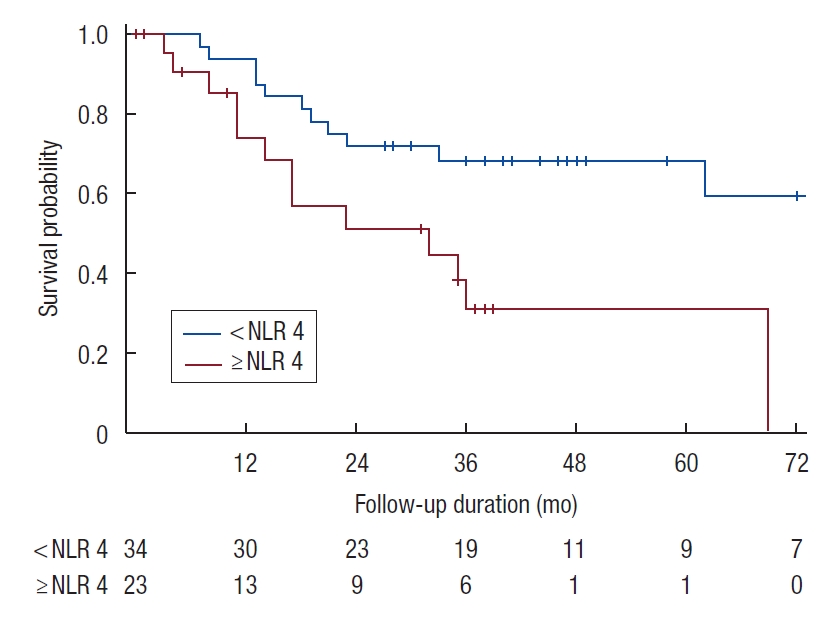
The median OS for the entire cohort was 70 months (range, 0 to 154 months) (Fig. 1), while the median RFS was 62 months (range, 3 to 154 months). The 5-year OS and RFS were 56% and 55%, respectively. H-NLR of ≥ 4 was significantly associated with poorer OS and RFS (P < 0.05) on univariate analysis (Figs. 2, 3).
Perineural infiltration, lymphovascular invasion, and absence of adjuvant chemotherapy were associated with worse OS on univariate analysis (Table 2). Major postoperative complication, of Clavien-Dindo grade III and above [17], and NLR of ≥ 4, negatively impacted OS on both univariate and multivariate analyses.
Among the factors associated with poorer RFS on univariate analysis—T4 tumors, perineural infiltration, lymphovascular invasion, and NLR of ≥ 4, perineural infiltration was found to be significant on multivariate analysis (Table 3).
DISCUSSION
The role of systemic inflammatory response in predicting oncological outcomes has been well demonstrated. In the presence of ongoing systemic inflammation, there is neutrophilia with a relative lymphocytopenia [18] due to elevation of proinflammatory tumor cells and suppression of cell-mediated immunity [19]. Markers used for inflammatory response include components of TWBC such as NLR, platelet-lymphocyte ratio, and lymphocytemonocyte ratio.
In particular, NLR has been shown to play an important role in predicting the survival of patients with different types of cancers [20], including breast [7], stomach [4], gastrointestinal stromal tumors [5], pancreatic [6] and hepatocellular carcinoma [21]. H-NLR has been correlated with cancer invasion, angiogenesis, and metastasis [22]. Indeed, a recent systemic review and meta-analysis by Dolan et al. [23] in 2017 showed that there was a significant association between NLR and OS in patients with operable cancer. The usefulness of NLR in the prognostication of CRC has been widely investigated [1, 8, 24-26]. Nevertheless to the best of our knowledge, the prognostic ability of NLR has not been examined among patients with obstructing CRC who have undergone endoscopic placement of SEMS as a bridge to curative surgery.
In this study, we show that elevated NLR is an independent prognostic factor associated with worse OS on both univariate and multivariate analyses. In addition, elevated NLR is significantly associated with worse RFS on univariate analysis. These findings are consistent with other studies which have reported the association of elevated NLR with adverse oncological outcomes including OS, cancer-specific survival, and RFS, in various cohorts of CRC patients [8, 25, 27, 28].
The NLR value of 4 after stenting was determined to be the most optimal threshold in differentiating survival outcomes in our study. Similarly, from the NLR values obtained at presentation before endoscopic stenting, the optimal value that best-dichotomized outcomes was 5. Both these NLR cutoff values, obtained before and after stent deployment, are consistent with the NLR threshold of between 3 to 5 reported in most studies examining the prognosticating value of NLR in CRC [23]. The effect of treatment of these obstructed patients with intravenous hydration and antibiotics is likely to account for the lower NLR threshold of 4 after endoscopic stent deployment. Therefore, the applicability of NLR as a simple and inexpensive biomarker-correlating inflammatory response to oncological outcomes [27, 29], can be extended to this subset of patients with obstructing localized CRC who are first decompressed by endoscopic stent placement followed by elective curative surgery.
Based on our cutoff value of 4, we found that elevated NLR after endoscopic stent placement was significantly associated with higher rates of apical lymph node involvement and lymphovascular invasion-pathologic indicators of adverse oncological outcome. Within the H-NLR group, the median CEA level was higher (7.75 vs. 4.50 μg/L) and there was a larger proportion of T4 tumors (30.4% vs. 14.7%), although these did not approach statistical significance. The 5-year OS and RFS of 56% and 55% respectively in our cohort. Similarly, a recent systemic review by Cao et al. [30] reported the 5-year OS ranging between 57% and 63% among patients with obstructing CRC.
The overall proportion of patients who completed adjuvant chemotherapy was 49.1% in this study, including 15 patients who declined further chemotherapy treatment postoperatively, whereas the remaining patients were unable to complete the full regimen due to side effects. While the proportion of patients in the H-NLR group vs. L-NLR group receiving chemotherapy were similar, there was a slightly higher rate of metachronous distant metastases observed among patients in the H-NLR group. With today’s emergence of more individualized treatment strategies, the oncologic prognostic significance of NLR can potentially aid the selection of our patients for adjuvant treatment or intensification of postoperative surveillance, in addition to the clinicopathological factors currently used.
The main limitations of this study are its retrospective nature and relatively small cohort size. Nonetheless, we demonstrate that the prognostic ability of NLR remains relevant among patients with obstructing localized CRC who are decompressed by endoscopic stent placement as a bridge to elective curative surgery.
In conclusion, NLR of ≥ 4 after stenting is an independent prognostic factor associated with worse OS and RFS, among patients with obstructing localized CRC who are decompressed by endoscopic stent placement as a bridge to elective curative surgery. NLR is a useful predictor of more advanced tumor biology, associated with higher rates of apical lymph node involvement and lymphovascular invasion.