INTRODUCTION
Cavernous hemangiomas of the colon are rare, benign vascular lesions, and the site most commonly affected is the rectosigmoid junction. Surgical treatment is recommended for large diffuse lesions but in the presence of pedunculated lesions, endoscopic resection should be preferred if possible.
We report a case of a 65-year-old man referred for colonoscopy after positive fecal occult blood.
CASE REPORT
A 65-year-old man with no relevant personal history and no usual medication was referred for colonoscopy after positive fecal occult blood test. He had no symptoms and blood tests revealed no signs of anemia or iron deficiency.
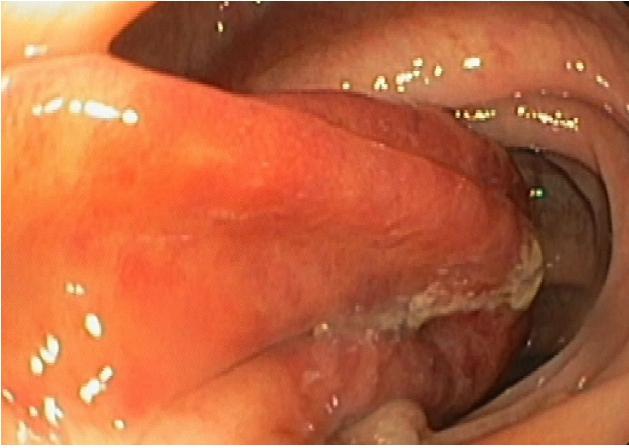
Colonoscopy was performed and revealed, at the level of the sigmoid colon, a wide base pedunculated polyp (35 mm) occupying more than half of the lumen, with the covering mucosa with a vinous appearance (Fig. 1).
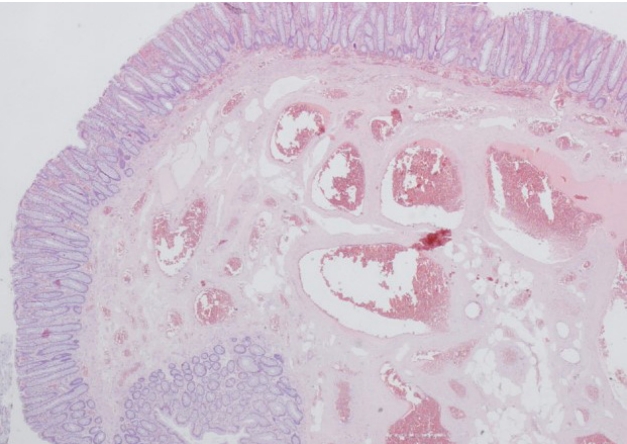
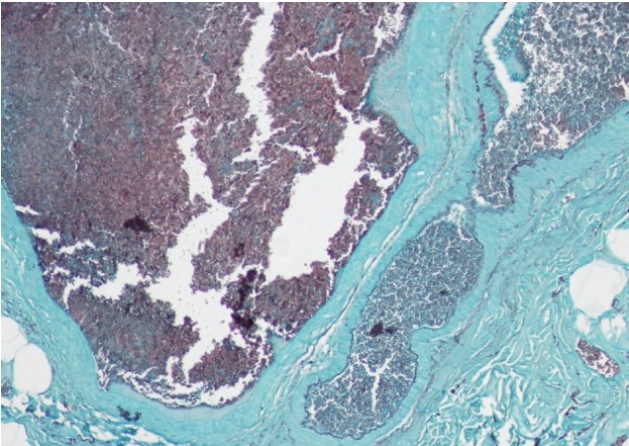
In order to remove the lesion, a detachable snare was placed and hot-snare polypectomy was performed. During the procedure, the detachable sna re was inadvertently cut, with active bleeding that was controlled after clip placement and diluted adrenaline injection (Fig. 2). The patient was admitted for surveillance after the procedure and was discharged after 1 day and did not have bleeding recurrence during the follow-up. The anatomopathological report described a polypoid lesion with hyperplastic mucosa and submucosal plane expanded by numerous thick-walled vessels in the context of cavernous colonic hemangioma (Figs. 3, 4). Colonoscopy was repeated after 3 months and the scar of the previous polypectomy was observed, without evidence of residual lesion.
DISCUSSION
Gastrointestinal hemangiomas are a rare, benign clinical entity that may present as overt or occult bleeding and can be distributed throughout the intestinal digestive system, or present as a singular cavernous hemangioma or malformation [1]. Regarding colonic cavernous hemangiomas the site most commonly affected is the rectosigmoid junction [2].
Colonoscopy is an invaluable tool, being both diagnostic and potentially therapeutic, with cyanoacrylate glue injection, endoscopic mucosal resection, and a variety of thermal modes, including argon plasma coagulation, being part of the therapeutic armamentarium that can possible be used to ablate this type of lesion [3]. Furthermore, there are case reports that validate endoscopic submucosal dissection as an efficient alternative for the complete removal of large colonic cavernous hemangiomas [4]. Surgical treatment is recommended for large diffuse lesions but in the presence of pedunculated lesions, endoscopic resection is a viable and less invasive option [5]. After a PubMed database search, we conclude that this is the second case report of successful removal of pedunculated colonic hemangioma by endoscopic snare polypectomy.
Endoscopic resection does have a significant probability of bleeding and a relevant bowel perforation risk, but it may constitute a less invasive alternative to surgery for smaller and focal vascular lesions such as cavernous hemangioma. For selected cases, we believe that endoscopic resection may have a therapeutic role, before contemplating surgery. Clinical surveillance after the procedure, as well as follow-up endoscopic surveillance, are essential to the safety and success of the procedure.
In the present case, the lesion did not have the typical angiomatous aspect, which may be explained by the presence of hyperplastic mucosal alterations with the presence of expanded vessels at the submucosa level. This case report highlights the importance of a careful endoscopic approach with adequate bleeding prophylaxis for the successful and safe removal of this lesion.