INTRODUCTION
Colonic duplication is a rare condition, representing the least common alimentary tract duplication. The cystic duplication type has been found to be more common than the tubular type in the colon [1]. Several theories have been postulated, but none are sufficiently well-accepted to explain the full spectrum of the disease.
Most duplications are found during surgery for another condition or incidentally on imaging studies. When symptomatic, the common complaints on presentation are chronic constipation, abdominal distension, or an abdominal mass [2]. A large proportion of symptomatic patients are diagnosed as toddlers, requiring surgery, but some remain asymptomatic and reach adulthood undiagnosed.
Surgery is the mainstay of treatment for colonic duplication, and throughout the years, multiple surgical interventions have been described. However, recent reports of malignancy in resected specimens highlight the importance of resection as the gold-standard treatment, especially in adult patients [3]. We report a case of a 23-year-old female patient with long-standing constipation who was eventually referred to us after computed tomography (CT) colonography found colonic duplication. The rarity of this case is seen in 3 aspects: the patient’s relatively old age at diagnosis, the colonic site, and long tubular type of involvement.
CASE REPORT
A 23-year-old woman reported that she had experienced chronic constipation since childhood. Her usual bowel habits were once a week to once a month. She described her bowel output as hard stools with no mucus or blood and spent more than an hour on the toilet during defecation. She reported occasional abdominal pain and distension but stated that she had not noticed any mass. She had sought medical advice for these symptoms since her teenage years but was often given laxatives without a proper full investigation. There was no other congenital deformity noted at birth or among her siblings and close relatives.
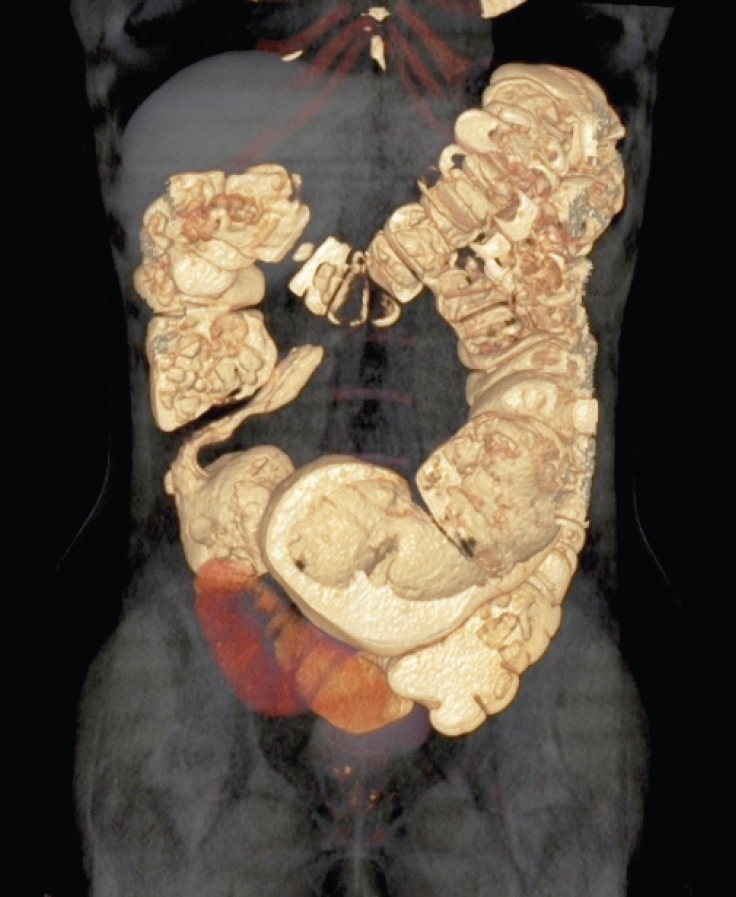
As her symptoms worsened in the past few months, she underwent colonoscopy after seeing a gastroenterologist. The colonoscopy was normal, and she was scheduled for a CT scan to explain her worsening symptoms. All of her biochemical investigations were normal. Full-thickness rectal biopsy revealed the presence of ganglionic cells in both the myenteric and submucosal plexuses. CT colonography showed a tubular colonic duplication from the transverse colon until the sigmoid colon, as demonstrated clearly on CT reconstruction (Fig. 1). No tumors or other duplications were noted involving any other part of the alimentary tract or other systems. She was then referred to Kolorektal Cerrahi Clinic (Izmir, Turkey) for further management and subsequently scheduled for surgery.
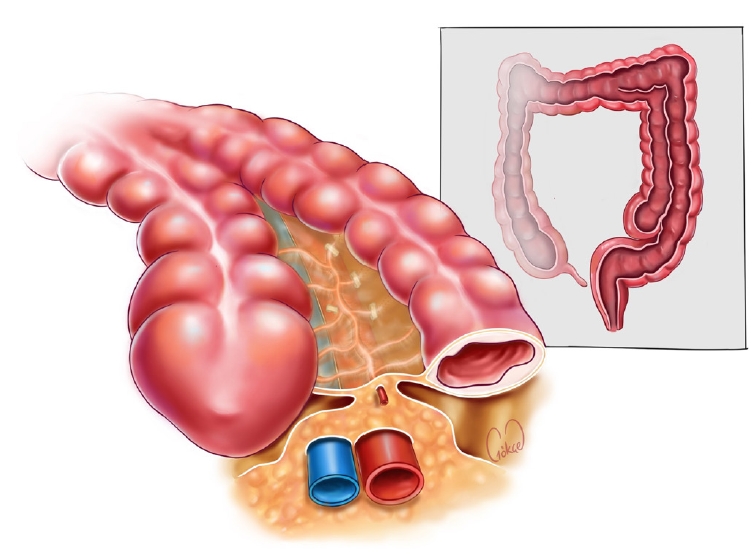
During laparoscopic exploration, a colonic duplication was seen, starting at the level of the mid-transverse colon, perpendicular to the middle colic vessels until the proximal sigmoid colon (Fig. 2). While ligating all appropriate vessels of the left colon, we observed that she had a short inferior mesenteric artery (IMA), which bifurcated, supplying both the native and duplicated sigmoid colon. This did not allow us to preserve this vessel, and high ligation of IMA was performed (Fig. 3). We decided to transect the right colon due to the short remaining segment of the right colon to perform a tension-free anastomosis in the pelvis. Intracorporeal stapled ileorectal anastomosis was performed after specimen extraction via a small transverse suprapubic incision. The patient recuperated well postoperatively and was discharged on day 4 after tolerating solids and having a bowel movement. A histopathological examination reported minimal fibrotic changes in the submucosal layer of the duplicated colon without any malignant changes.
This study was approved by the Institutional Review Board of Kent Hospital (Izmir, Turkey; No. KH2023/216). The patient provided written informed consent for the publication of the research details and clinical images.
DISCUSSION
Alimentary tract duplication is a congenital deformity reported in 1 in every 4,500 births, most commonly in the terminal ileum [1]. The hallmark of colonic duplication is that it must be within the proximity of the colon, its wall must be continuous with the native colon, with the myenteric cells and smooth-muscle layers present, and it must be lined by alimentary epithelium, although not supposedly colonic epithelium [3]. McPherson et al. [4] further classified these duplications into 3 types, separating them according to their association with the native colonic wall and the size or extent of the duplicated segment. The mesenteric cyst type, only found on the mesenteric side of the colon, has minimal or no continuation with the colonic wall, but is still lined with intestinal epithelium and smooth muscle. The diverticular type can also be found in the antimesenteric side and connects with the normal colon in part or all of its length. Long colon duplication is explained as a rare type, usually involving the majority or entire length of the colon and rectum and sharing the same wall throughout. Smith [5] proposed a simpler stratification, dividing duplications into spherical and tubular according to their size and form. Spherical forms are identical to a diverticulum, while the latter type usually involves a long segment of the colon, both with almost exact wall formation with its native tract. A frequently observed histopathological finding of cystic duplication is the presence of heterotopic tissues, such as gastric or pancreatic cells.
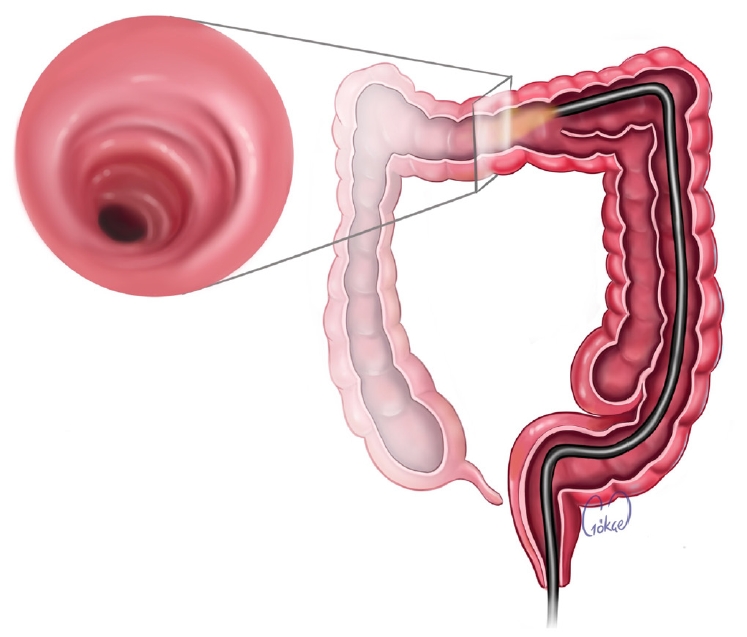
Colonoscopy has always been part of the workup for patients with chronic constipation. Although it is considered a useful investigation, a straight view of colonoscope may still miss the intraluminal features of a duplication in the colon due to its technical limitations (Fig. 4). Colonoscopy failed to detect our patient’s condition; however, CT colonography with its reconstructed images helped to confirm the diagnosis.
In colonic duplication, unlike other similar alimentary tract deformities, surgical intervention involving bowel resection and anastomosis is a favored treatment, whether it is found unintentionally during exploration or on an elective basis, except in asymptomatic pediatric patients. Several reports have also suggested the role of enucleation and unroofing in these pediatric age groups [6]. The main reason for resection of the duplicated segment is the risk of developing malignancy from the duplicated mucosa. Reviews of pathology reports after the resection of duplicated colons reported a 7% to 10% risk of malignant transformation. This percentage is highest in colorectal duplication than in duplication along other parts of the gastrointestinal tract. Studies have suggested that the duplicated epithelium carries a high risk of carcinogenesis [7, 8]. Fecal matter moves more slowly through a duplicated segment, which explains the common symptoms of chronic constipation and delayed transit time. This may be the cause of the increased risk of carcinogenesis in the bowel mucosa as well.
Adenocarcinoma is the most common histological type of cancer found in cases of colonic duplication, but there have also been reports of squamous cell carcinoma, gastrointestinal stromal tumor, carcinoid tumor and leiomyosarcoma [9, 10]. Carcinoembryonic antigen (CEA) levels could be an indicator of the presence of malignancy in a duplicated colon. Reports have suggested that elevated CEA levels are present in a higher proportion of duplicated colon carcinomas than in usual colorectal cancer patients. Patients presenting with abdominal pain or a palpable mass should be screened routinely for CEA, since this information could help in surgical decision-making and the determination of whether excision should be done for oncological clearance [11, 12]. Beyond the risk of cancer, other possible complications such as perforation, bleeding, and obstruction have been described, even among the early cases reported, as potential causes of mortality. This factor tilts the favored management towards surgery when diagnosed early. We hereby emphasize the need for colonic resection, as seen in our patient, who underwent subtotal colectomy. This was the most appropriate management in view of her age and the risk that this condition carries.
Laparoscopic surgery was introduced in the late 20th century, but not until the turn of the century was it reported to be used for alimentary tract duplication [13]. Li et al. [7] reported in their paper on all colonic duplication cases published until 2020 that laparoscopic surgery has been used in about 10% of cases from then on. The postoperative recovery was uneventful in all of those patients, who fully benefited from the advantages of laparoscopic surgery. They went on to suggest that asymptomatic patients undergoing elective surgery must be offered minimally invasive surgery in available centers. In a retrospective multicenter review of gastrointestinal duplication in pediatric patients treated with minimally invasive surgery, only 1 of 4 cases of colonic duplication was converted to open laparotomy during exploration [14]. Our patient had been accurately diagnosed from the investigations that had been done and planned for elective surgery; thus, minimally invasive laparoscopic surgery was deemed to be the most appropriate option, given its benefits.
The options for surgical excision generally depend on the anatomical type. According to the classification of McPherson et al. [4], the mesenteric cyst and diverticular types can easily be dealt with by simple excision or wedge resection of the native colon. Previous reports have also suggested excising the duplicated segment without resecting any part of the native colon [9]. Recent reports have also described successfully resecting rectal duplication cysts through the transanal approach. The main principle of excision should generally be to avoid any vascular compromise or any bowel wall defect/abnormality of the native colon as a result of removing the duplicated segment [1]. We noted a short IMA bifurcation supplying both the duplicated and native sigmoid colon in our patient. In keeping with the above principle, we needed to ligate and divide this main vessel, resecting the whole length of the sigmoid colon and creating an ileorectal anastomosis.
In long colonic duplication, resection must be done together with the native colon because of the close proximity and shared blood supply. It is also important to remember to add a proximal and distal margin of at least 2 cm of the normal bowel upon bowel resection. This is based on pathological reports of the presence of fibrotic tissues at the junction where the duplicated segment arises and ends, which will compromise healing if anastomosis is done at this site. This is even more important if malignancy is suspected [15]. Our patient had a long colonic duplication extending from the mid-transverse colon until the sigmoid colon, and the decision for total colectomy was the best for her in view of an easier positional tension-free ileorectal anastomosis compared to an ascending colon-rectum anastomosis.
Colonic duplication is often diagnosed in childhood, although some people with this condition may progress into adulthood undiagnosed due to its nonspecific symptoms and diagnostic dilemmas. Forward viewing of colonoscopy may not detect the duplication, so a low threshold of suspicion for performing CT colonography may be helpful. The surgical management of this condition is excision, and the long tubular type requires en bloc resection with its native colon to avoid complications and malignancy.