INTRODUCTION
Mixed adenoneuroendocrine carcinomas (MANECs) are rare tumors arising in the gastrointestinal (GI) tract composed of adenocarcinoma and neuroendocrine carcinoma (NEC) and have been defined as a carcinoma of the appendix arising from a preexisting goblet cell carcinoid (GCC) tumor [1]. MANECs have been reported to occur in the GI tract, pancreas, gallbladder, and uterine cervix. Malignancies of the appendix account for about 1% of all GI neoplasms and mainly represent neuroendocrine neoplasms and carcinomas. MANEC is rarely misdiagnosed as adenocarcinoma. If pathologists do not demonstrate the neuroendocrine morphology of the tumor in routine hematoxylin-eosin staining, then there is a danger of overlooking NEC of the colon and rectum. Because immunohistochemical staining cannot be performed for all carcinomas of the colon and rectum, pathologists should pay attention to the neuroendocrine morphology and actively perform immunohistochemical staining [2]. The 2010 World Health Organization (WHO) classification of appendiceal tumors recognized 2 separate entities; classic GCCs and MANECs [1]. While GCCs comprise well-defined goblet cell clusters with mild to moderate atypical cells, MANECs are composed of more aggressive tumor cells. Also, MANECs have a much worse prognosis than GCCs and are usually recognized by peritoneal dissemination [1, 3]. According to the 2017 WHO classification reported later, adenocarcinomas other than neuroendocrine tumors or MANECs that exhibit NEC-like genomic alterations probably reflect clonal evolution within tumors, a rapidly growing area of interest. Because of this, studies of these mixed carcinomas may also improve our understanding of other aspects of clonality in tumors of the digestive system and other parts of the body [4]. MANECs as well as NEC usually require more complex management, including chemotherapy. The curative treatment is known as surgical resection. However, since this disease is often diagnosed very late, the prognosis is reported to be poor [2].
Here, we report a MANEC of the appendix with peritoneal metastasis that was misdiagnosed as sigmoid colon (S-colon) cancer with peritoneal seeding and was treated with cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC).
CASE REPORT
A 61-year-old man visited a local hospital presenting with abdominal distention with no other symptoms. The patient had no specific past medical history. Abdominopelvic computed tomography (APCT) revealed irregular wall thickening with luminal narrowing at the distal S-colon and omental seeding with a large amount of ascites. Also, pleural effusion was found on APCT imaging. Colonoscopy revealed acute angulation of the distal descending colon, 40 cm above the anal verge, making further insertion impossible. There was no definite tumor lesion, and an endoscopic biopsy of the colon was taken, revealing nonspecific changes in the normal colon. The positron emission tomography (PET) examination showed no clear uptake in the intestine or solid organ, but uptake in the omentum was confirmed, suggesting peritoneal seeding. Although the endoscopic findings were not clear, APCT findings showed that the bowel wall of the S-colon was thickened, suggesting a malignant disease of the S-colon. The PET-CT showed no uptake in the bowel, but the uptake in the omentum showed that seeding was suspected. The clinical diagnosis was S-colon cancer with peritoneal metastasis, and diagnostic laparoscopy was performed. Only laparoscopic peritoneal biopsy was performed, and definitive surgery was not performed because of disseminated peritoneal and omental seeding. The pathology was mainly signet ring cell carcinoma with focal mucinous carcinoma components. Furthermore, CK7, CK19, CK20, and CDX-2 results were strongly positive on the immunohistochemistry. The tumor was confirmed to be KRAS wild type. And NRAS gene mutation was not observed, and epidermal growth factor receptor mutation was positive. So, the patient underwent palliative treatment with FOLFIRI (folinic acid, fluorouracil, and irinotecan) and cetuximab given a diagnosis of colon cancer with peritoneal seeding.
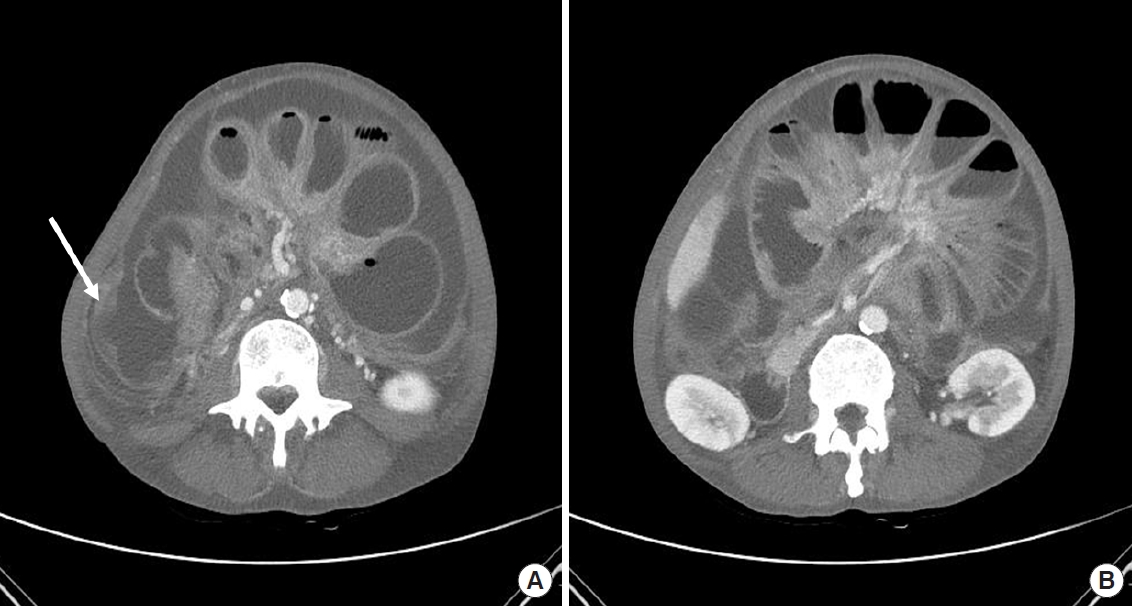
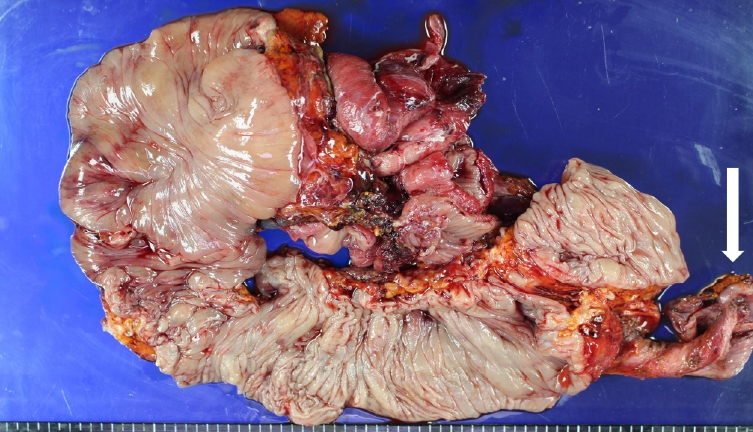
After 2 cycles of chemotherapy, the patient still complained of nausea, vomiting, and abdominal distension. Small bowel obstruction by malignant seeding was suspected on APCT (Fig. 1). His general condition was very poor because he could not eat. After 2 weeks of conservative treatment, the second surgery was performed, which was 3 months after the first surgery. Omentum conglomeration by intraperitoneal seeding was observed, and seeding nodules were disseminated in the small bowel mesentery and peritoneum. An obstruction was also found at the proximal site of the ileum. The peritoneal metastasis was spread throughout the abdominal cavity, and each seeding mass was of various sizes and was heavily agglomerated in the mesentery of the small intestine. A conglomerate peritoneal metastatic lesion was causing obstruction of the small intestine. About 200 mL of translucent colored mucus was also observed in the abdominal cavity. The intraoperative peritoneal cancer index score was confirmed to be 32 points. We performed a total peritonectomy, a total colectomy including the ileum obstruction site, and carried out a permanent ileostomy. The postoperative specimen photos can be seen in Fig. 2. All metastatic lesions in the peritoneum were removed. However, the seeding lesion existing in the mesentery of the small intestine and large intestine was removed as much as possible, but it was thought to remain about 2 cm in size, so it was checked with the completeness of cytoreduction rate (CCR2). Immediately after the abdomen was closed, HIPEC was maintained for 60 minutes with 2 L of 1.5% dextrose dialysis solution warmed at 42 °C that was mixed with 30 mg of mitomycin C. After that, 10 mg of mitomycin C was added for an additional 30 minutes. HIPEC, which is performed during surgery at our hospital, uses the same dose regardless of the patient’s weight. The total operation time was 625 minutes.
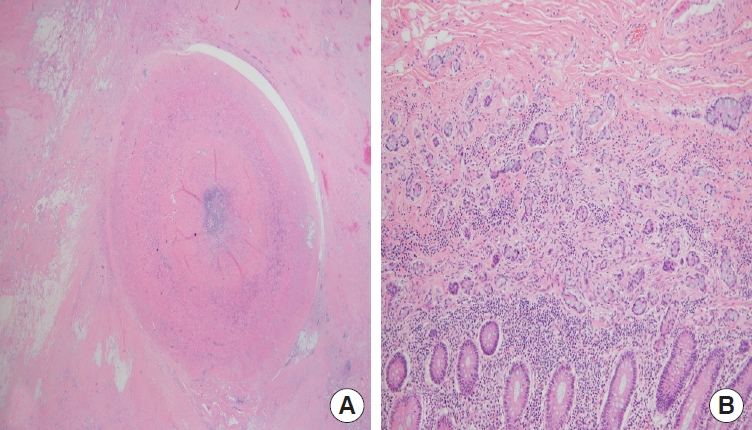
Three days after surgery, we started early postoperative intraperitoneal chemotherapy (EPIC) with 5-fluorouracil (15 mg/kg) that was mixed with 800 mL of 1.5% dextrose dialysis solution; the solution was drained after 23 hours in intraperitoneum, and EPIC was repeated for 4 days. The patient had a slight bleeding tendency and mild ileus until the second day after surgery, so EPIC was performed from the third day after the operation, when these symptoms improved. In our hospital principle, if there is no special event after surgery, EPIC is performed from the day after surgery. The tube for intraperitoneal injection uses a catheter for peritoneal dialysis known as a continuous ambulatory peritoneal dialysis catheter. And the tube for draining the intraperitoneal anticancer drug uses 4 area Jackson-Pratt drain catheters that are placed during surgery. The pathologist reported a 1.5 × 3.0 cm MANEC on the appendix that had perforated the visceral peritoneum without regional lymph node metastasis (Fig. 3). Also, multiple intraperitoneal metastases were confirmed (Fig. 4).
The patient started intravenous chemotherapy with FOLFOX (folinic acid, fluorouracil, and oxaliplatin) 35 days after surgery. He was discharged once he could ingest a soft diet with little discomfort. The patient was hospitalized for a total of 49 days and was discharged on the 35th day after surgery. No postoperative complications were observed in the patient until discharge. After surgery, FOLFOX was administered up to 12 times, and pneumonia developed right after the end of chemotherapy, and he died 9 months after surgery due to lung failure.
DISCUSSION
Despite the disparity in their prognosis, MANECs and GCCs have been historically reported as adenocarcinoids or GCCs because of the presence of goblet cell clusters. Early studies of adenocarcinoids reported mostly in the 1970s and 1980s pointed to the intermediate features and prognosis of typical appendiceal carcinoids and colonic adenocarcinomas as well as their spectrum of goblet cell cluster percentages, mucine amounts, nuclear atypia, mitotic counts, and metastatic ability [5–12] .
Tang et al. [3] classified 63 cases of appendiceal adenocarcinoids into 3 categories; typical GCC (group A), adenocarcinoma ex-GCC subtype signet ring cell (group B), and poorly differentiated adenocarcinoma ex-GCC subtype (group C). The extracellular mucin can be prominent in groups A and B. Additionally, all groups presented focal immunoreactivity for neuroendocrine markers (chromogranin or synaptophysin mainly); however, while groups A and B showed normal expression levels of intestinal mucin glycoproteins (MUC1−/MUC2+) and Ki67 of <20%, group C had abnormal p53 expression, β-catenin immunoreactivity, a MUC1+/MUC2− pattern, and Ki67 of >70%. In the 2010 WHO classification, group A is referred to as a GCC group, and groups B and C are referred to as MANEC groups [1].
Staging is based on the colonic adenocarcinoma staging system from the American Joint Committee on Cancer (AJCC) [13]. Most patients with GCCs (63%) presented metastasis at the time of diagnosis. The tumor stage correlated to the histologic grade of the primary tumor. Accordingly, 33% of group A, 88% of group B, and 100% of group C had metastases at the time of initial presentation. Specifically, the overall disease-specific survival of group A was 96%, that of group B was 73%, and that of group C was 14% during follow-up. Both the 3- and 5-year disease-specific survival rates of group A were 100%, while these rates were 85% and 36% in group B and 17% and 0% in group C, respectively [3]. The mean survival of GCCs is 47 months, with an overall 5-year survival rate of 45%. Aggressive surgical CRS and chemotherapy may be viable option to manage peritoneal seeding. Brathwaite et al. [14] conducted a population-based study of SEER (Surveillance, Epidemiology, and End Results) on appendiceal MANEC. According to his argument, patients with MANEC undergo aggressive multidisciplinary oncology management that may include systemic therapy and well-selected aggressive surgical management. Right hemicolectomy has been considered a standard treatment in the management of GCCs and MANECs in the appendix. However, in the case of signet ring cell adenoneuroendocrine carcinomas, pT3/pT4, perforated appendix tumors, or positive margins in the appendectomy, right hemicolectomy is the recommended option, followed by intravenous chemotherapy, in stage III disease. In addition, in cases of poorly differentiated adenoneuroendocrine carcinomas or cases with intraperitoneal spread, CRS plus HIPEC followed by intravenous chemotherapy is recommended [3]. In addition, as in this case, the possibility of recurrent intestinal obstruction is very high. End ileostomy was unavoidably performed rather than an intestinal anastomosis because there is a possibility that intestinal obstruction may occur again in the future due to peritoneal metastasis remaining in the abdominal cavity. HIPEC is a new option for neoplasms with frequent peritoneal spreading carcinomatosis, which is the main cause of death in these patients [10, 15]. There is still insufficient evidence to implement a complex and invasive treatment such as CRS-HIPEC for peritoneal metastasis caused by MANEC as in this patient. However, although not many, there are studies and case reports showing positive results on the effect of CRS-HIPEC due to peritoneal metastasis of MANEC [16, 17]. The effect of surgical and chemotherapeutic interventions on survival was examined. Right hemicolectomy did not improve the survival rate for stage IV patients. Aggressive surgical debulking to decrease tumor burden has been shown to improve survival in ovarian neoplasms and appendiceal mucinous cystadenocarcinoma. However, CRS surgery without HIPEC should be avoided because it may miss the opportunity to receive other combination treatments for better results in the future. Resection of peritoneum without HIPEC allows free tumor cells to implant and grow all over the abdominal cavity, which impairs future treatment options and increases the risk of morbidity. The use of intravenous chemotherapy has been explored through several case reports using different drugs. The usual schemes include those used for colonic adenocarcinomas, which include 5-fluorouracil, leucovorin, oxaliplatin, and irinotecan [3, 15]. Similar to typical NECs, schemes with cisplatin plus etoposide or 5-fluorouracil, cisplatin, and streptozotocin have also been used [18].
According to the study of Sluiter et al. [16], treatment with CRS-HIPEC for patients with peritoneal metastases of GCCs and MANECs in specialized HIPEC centers seems associated with substantially better outcome compared to surgery without HIPEC at the expense of acceptable morbidity and mortality. And these data support that care of patients with peritoneal metastases of GCCs and MANECs should be offered in expert centers that have the option for CRS-HIPEC.
In conclusion, MANEC arising from the appendix is a very rare malignancy that behaves aggressively and usually presents with peritoneal spreading. The origin site of the primary tumor can be difficult to determine. Thus, if some patients with aggressive peritoneal spreading present without a clear primary site, then appendectomy may help identify the site of origin. Also, advanced-stage patients with peritoneal spreading of carcinomatosis can be managed with CRS with HIPEC, usually followed by intravenous chemotherapy and EPIC.